

A narrative review on characterization of acute respiratory distress syndrome in COVID-19-infected lungs using artificial intelligence
- PMID: 33550068
- PMCID: PMC7813499
- DOI: 10.1016/j.compbiomed.2021.104210
A narrative review on characterization of acute respiratory distress syndrome in COVID-19-infected lungs using artificial intelligence
Abstract
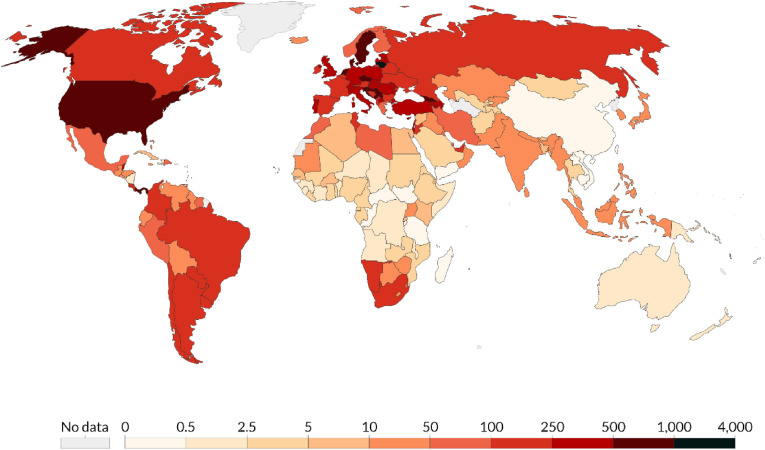
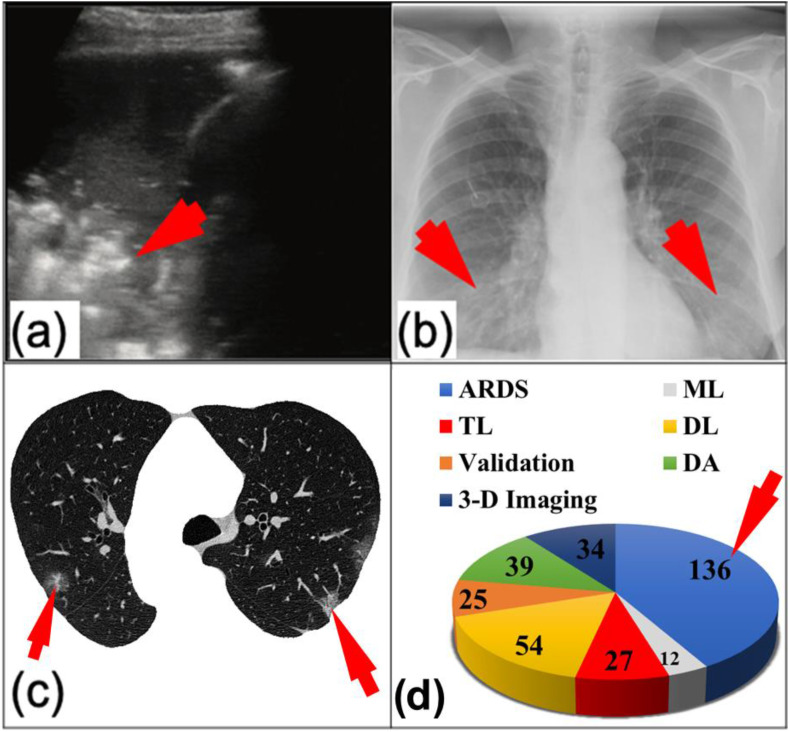
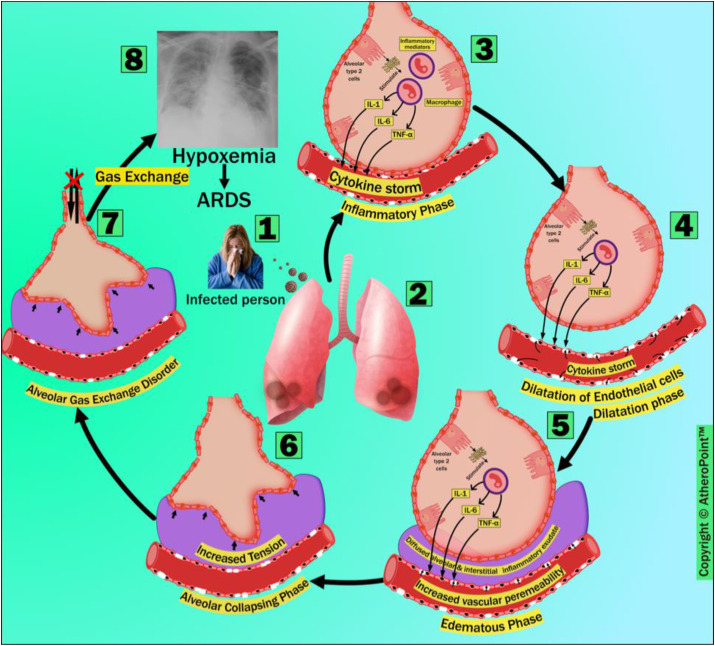
COVID-19 has infected 77.4 million people worldwide and has caused 1.7 million fatalities as of December 21, 2020. The primary cause of death due to COVID-19 is Acute Respiratory Distress Syndrome (ARDS). According to the World Health Organization (WHO), people who are at least 60 years old or have comorbidities that have primarily been targeted are at the highest risk from SARS-CoV-2. Medical imaging provides a non-invasive, touch-free, and relatively safer alternative tool for diagnosis during the current ongoing pandemic. Artificial intelligence (AI) scientists are developing several intelligent computer-aided diagnosis (CAD) tools in multiple imaging modalities, i.e., lung computed tomography (CT), chest X-rays, and lung ultrasounds. These AI tools assist the pulmonary and critical care clinicians through (a) faster detection of the presence of a virus, (b) classifying pneumonia types, and (c) measuring the severity of viral damage in COVID-19-infected patients. Thus, it is of the utmost importance to fully understand the requirements of for a fast and successful, and timely lung scans analysis. This narrative review first presents the pathological layout of the lungs in the COVID-19 scenario, followed by understanding and then explains the comorbid statistical distributions in the ARDS framework. The novelty of this review is the approach to classifying the AI models as per the by school of thought (SoTs), exhibiting based on segregation of techniques and their characteristics. The study also discusses the identification of AI models and its extension from non-ARDS lungs (pre-COVID-19) to ARDS lungs (post-COVID-19). Furthermore, it also presents AI workflow considerations of for medical imaging modalities in the COVID-19 framework. Finally, clinical AI design considerations will be discussed. We conclude that the design of the current existing AI models can be improved by considering comorbidity as an independent factor. Furthermore, ARDS post-processing clinical systems must involve include (i) the clinical validation and verification of AI-models, (ii) reliability and stability criteria, and (iii) easily adaptable, and (iv) generalization assessments of AI systems for their use in pulmonary, critical care, and radiological settings.
Keywords: ARDS; Artificial intelligence; COVID-19; CT; Comorbidity; Deep learning; Machine learning; Medical imaging; Transfer learning; US; Ultrasound; X-ray.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
We wish to confirm that there are no known conflicts of interest associated with this publication and there has been no significant financial support for this work that could have influenced its outcome. We confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed. We further confirm that the order of authors listed in the manuscript has been approved by all of us.
We confirm that we have given due consideration to the protection of intellectual propertyassociated with this work and that there are no impediments to publication, including thetiming of publication, with respect to intellectual property. In so doing we confirm that we have followed the regulations of our institutions concerning intellectual property.
We understand that the Corresponding Author is the sole contact for the Editorial process. He is responsible for communicating with the other authors about progress, submissions of revisions and final approval of proofs. We confirm that we have provided a current, correct email address which is accessible by the Corresponding Author and which has been configured to accept email from.”
I, Mainak Biswas on behalf of all authors of the manuscript “
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
