

Gut microbiota development during infancy: Impact of introducing allergenic foods
- PMID: 33551026
- PMCID: PMC9169695
- DOI: 10.1016/j.jaci.2020.09.042
Gut microbiota development during infancy: Impact of introducing allergenic foods
Abstract
Background: The gut microbiota potentially plays an important role in the immunologic education of the host during early infancy.
Objective: We sought to determine how the infant gut microbiota evolve during infancy, particularly in relation to hygiene-related environmental factors, atopic disorders, and a randomized introduction of allergenic solids.
Methods: A total of 1303 exclusively breast-fed infants were enrolled in a dietary randomized controlled trial (Enquiring About Tolerance study) from 3 months of age. In this nested longitudinal study, fecal samples were collected at baseline, with additional sampling of selected cases and controls at 6 and 12 months to study the evolution of their gut microbiota, using 16S ribosomal RNA gene-targeted amplicon sequencing.
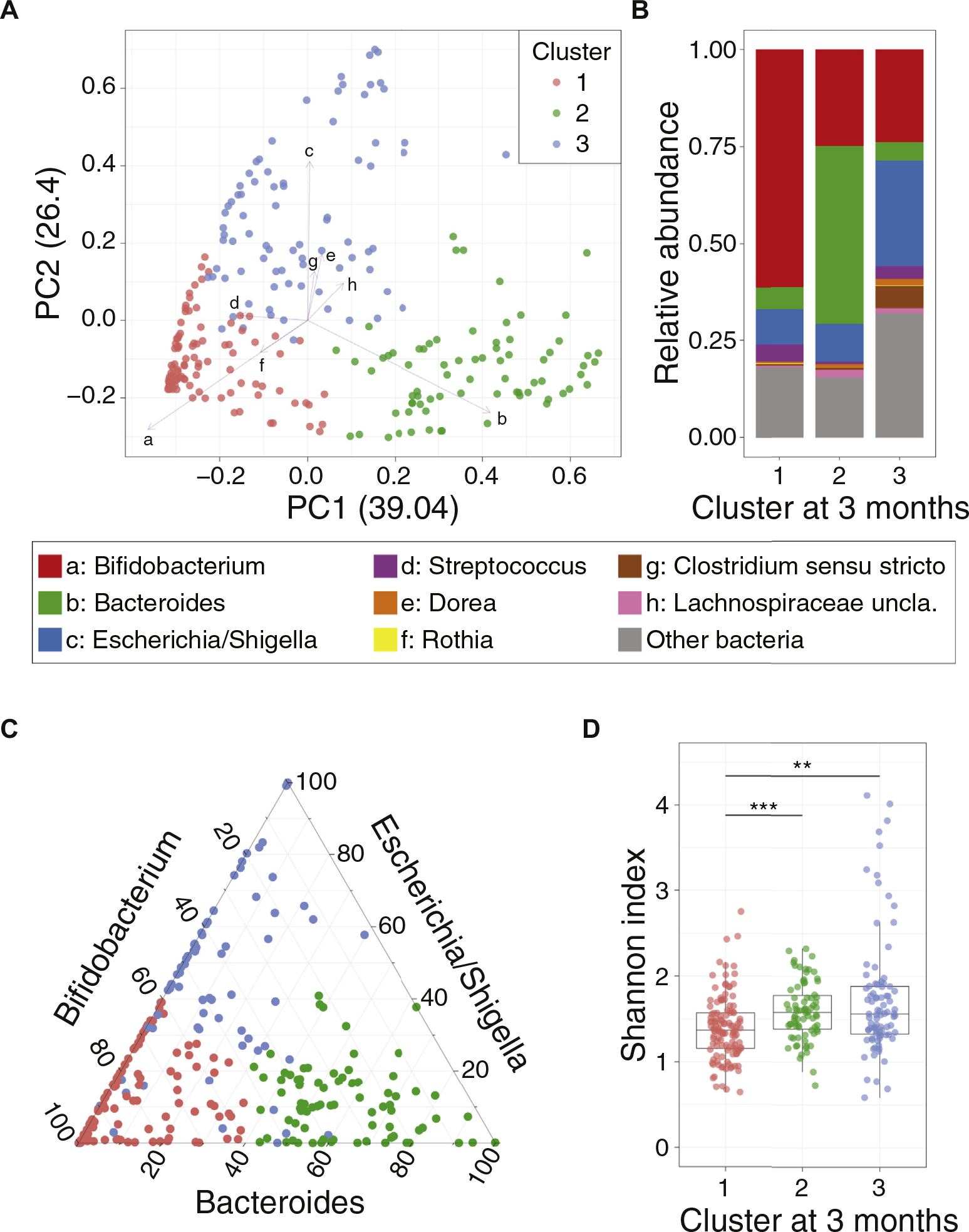
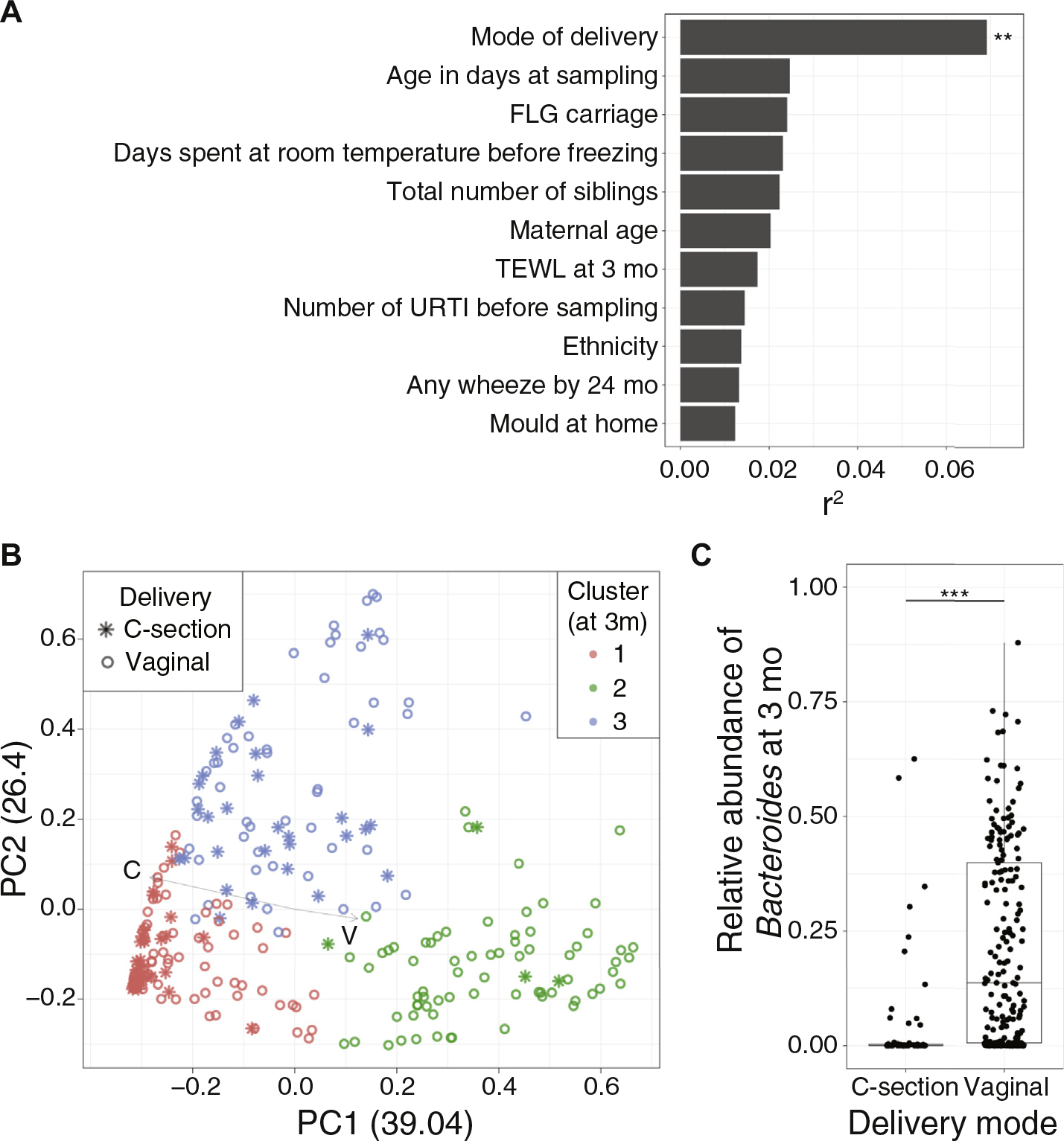
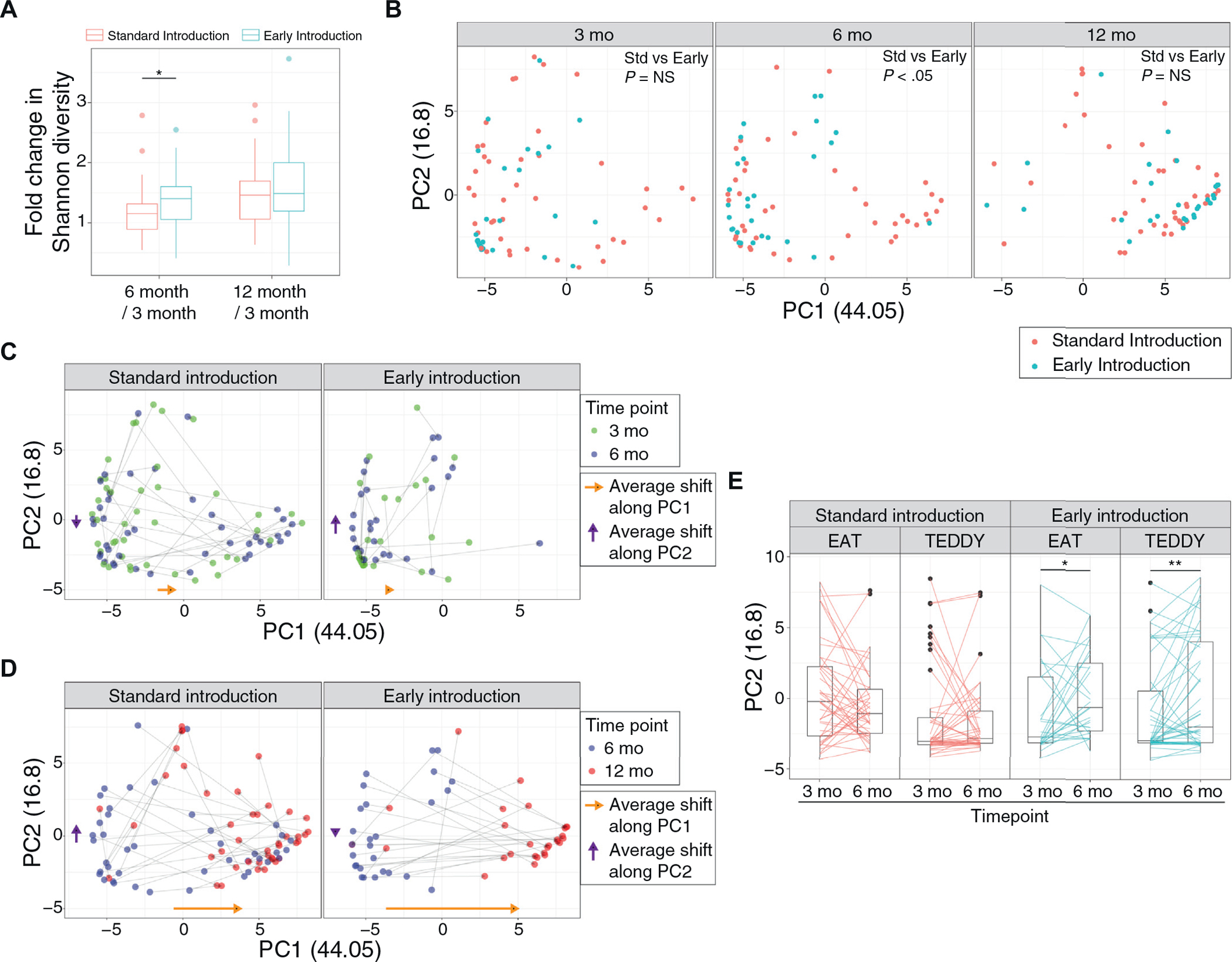
Results: In the 288 baseline samples from exclusively breast-fed infant at 3 months, the gut microbiota was highly heterogeneous, forming 3 distinct clusters: Bifidobacterium-rich, Bacteroides-rich, and Escherichia/Shigella-rich. Mode of delivery was the major discriminating factor. Increased Clostridium sensu stricto relative abundance at 3 months was associated with presence of atopic dermatitis on examination at age 3 and 12 months. From the selected cases and controls with longitudinal samples (n = 70), transition to Bacteroides-rich communities and influx of adult-specific microbes were observed during the first year of life. The introduction of allergenic solids promoted a significant increase in Shannon diversity and representation of specific microbes, such as genera belonging to Prevotellaceae and Proteobacteria (eg, Escherichia/Shigella), as compared with infants recommended to exclusively breast-feed.
Conclusions: Specific gut microbiota characteristics of samples from 3-month-old breast-fed infants were associated with cesarean birth, and greater Clostridium sensu stricto abundance was associated with atopic dermatitis. The randomized introduction of allergenic solids from age 3 months alongside breast-feeding was associated with differential dynamics of maturation of the gut microbial communities.
Keywords: Atopic dermatitis; bacteria; colonization; diet; environment; food; microbiome; tolerance.
Copyright © 2020. Published by Elsevier Inc.
Figures
References
-
- Zeissig S, Blumberg RS. Life at the beginning: perturbation of the microbiota by antibiotics in early life and its role in health and disease. Nat Immunol 2014;15: 307–10. - PubMed
-
- Arrieta MC, Stiemsma LT, Dimitriu PA, Thorson L, Russell S, Yurist-Doutsch S, et al. Early infancy microbial and metabolic alterations affect risk of childhood asthma. Sci Transl Med 2015;7:307ra152. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
