

Composite Epstein-Barr Virus-associated T-lymphoblastic and Peripheral T-cell Lymphomas: A Clonal Study
- PMID: 33551410
- PMCID: PMC8313923
- DOI: 10.2169/internalmedicine.6572-20
Composite Epstein-Barr Virus-associated T-lymphoblastic and Peripheral T-cell Lymphomas: A Clonal Study
Abstract
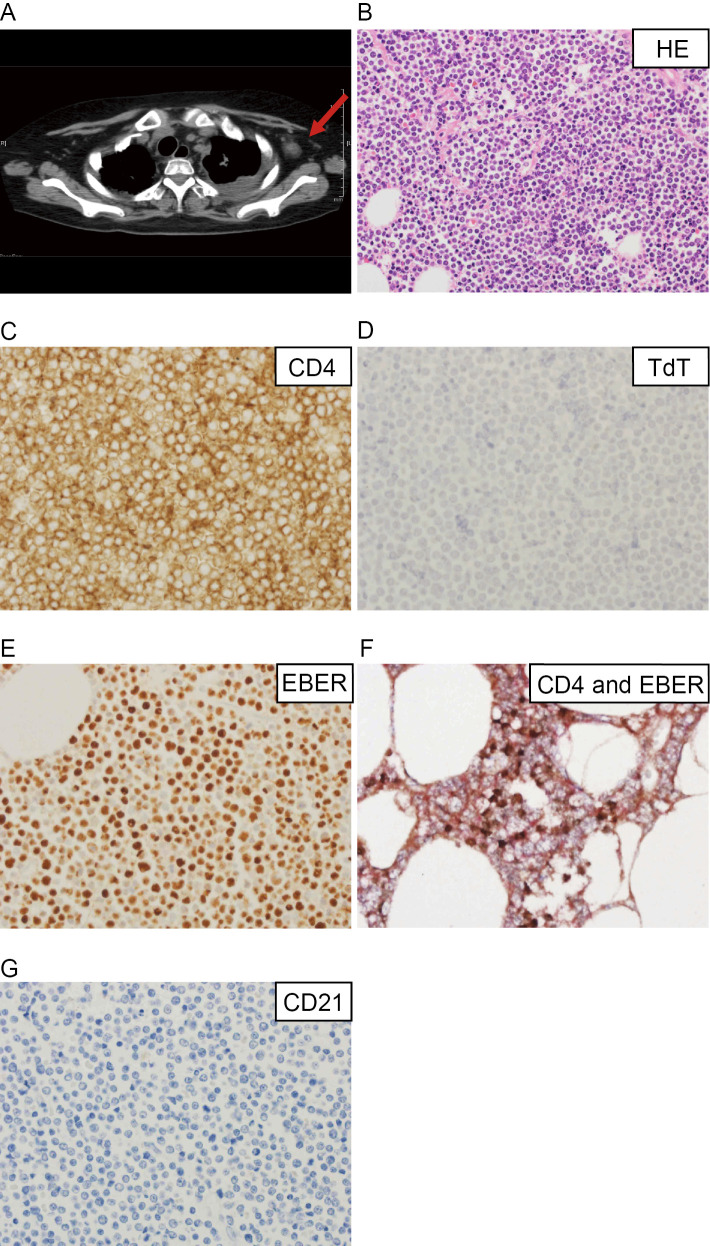
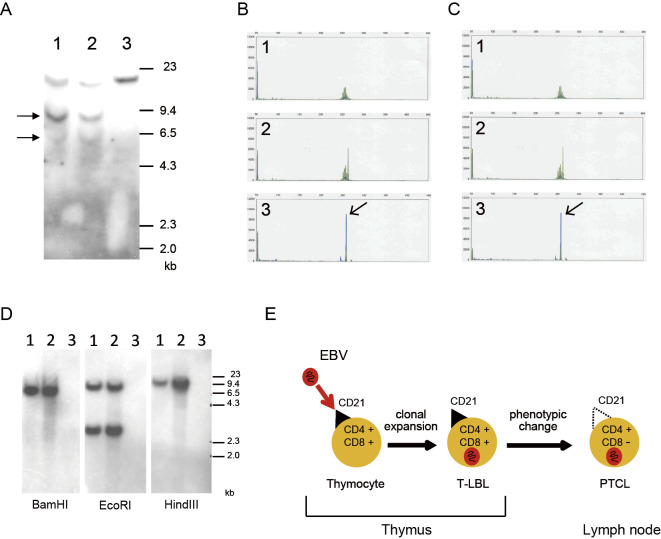
A 30-year-old woman was diagnosed with T-lymphoblastic lymphoma (T-LBL) that harbored a clonal Epstein-Barr virus (EBV) genome. At relapse, axillary lymph node adenopathy, which was diagnosed as peripheral T-cell lymphoma, not otherwise specified (PTCL-NOS), was detected. Southern blot analyses of the T-cell receptor and EBV genome revealed that the T-LBL and PTCL-NOS were clonally identical. We previously showed that CD21 acted as an entry molecule that allowed EBV into the patient's T-LBL cells. Interestingly, the PTCL-NOS cells lacked CD21 expression. Our case suggests that EBV might infect immature CD21-positive T-cells, and CD21-negative PTCL-NOS might subsequently arise through phenotypic changes.
Keywords: CD21; Epstein-Barr virus; T-lymphoblastic lymphoma; composite lymphoma; peripheral T-cell lymphoma.
Conflict of interest statement
Figures
References
-
- Young LS, Yap LF, Murray PG. Epstein-Barr virus: more than 50 years old and still providing surprises. Nat Rev Cancer 16: 789-802, 2016. - PubMed
-
- Braun M, Melchers I, Peter HH, Illges H. Human B and T lymphocytes have similar amounts of CD21 mRNA, but differ in surface expression of the CD21 glycoprotein. Int Immunol 10: 1197-1202, 1998. - PubMed
-
- Castillo JJ, Reagan JL, Bishop KD, Apor E. Viral lymphomagenesis: from pathophysiology to the rationale for novel therapies. Br J Haematol 165: 300-315, 2014. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources