

Development of a Fast SARS-CoV-2 IgG ELISA, Based on Receptor-Binding Domain, and Its Comparative Evaluation Using Temporally Segregated Samples From RT-PCR Positive Individuals
- PMID: 33552028
- PMCID: PMC7854536
- DOI: 10.3389/fmicb.2020.618097
Development of a Fast SARS-CoV-2 IgG ELISA, Based on Receptor-Binding Domain, and Its Comparative Evaluation Using Temporally Segregated Samples From RT-PCR Positive Individuals
Abstract
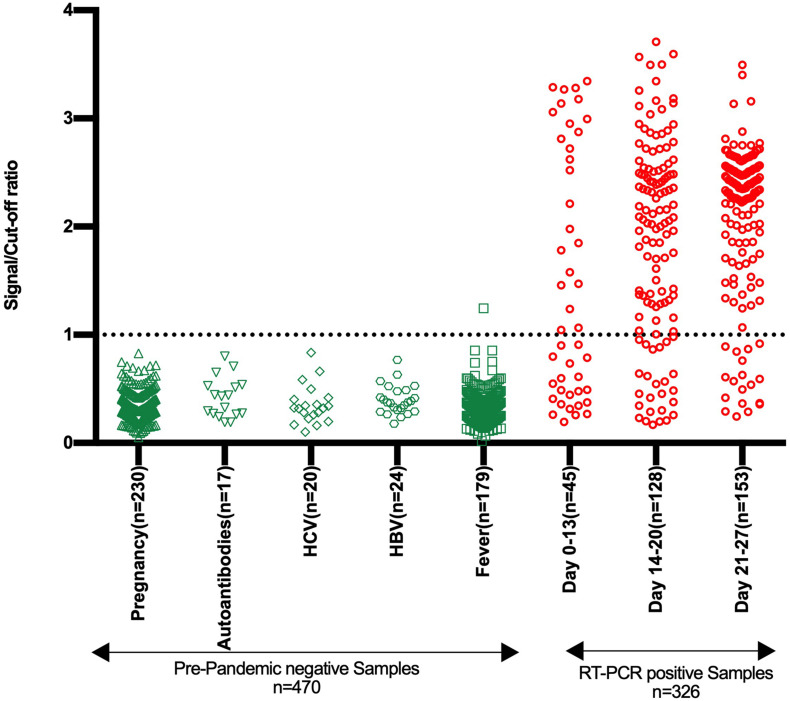
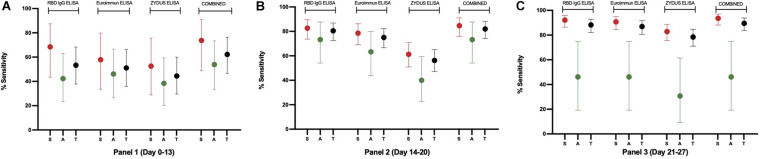
SARS-CoV-2 antibody detection assays are crucial for gathering seroepidemiological information and monitoring the sustainability of antibody response against the virus. The SARS-CoV-2 Spike protein's receptor-binding domain (RBD) is a very specific target for anti-SARS-CoV-2 antibodies detection. Moreover, many neutralizing antibodies are mapped to this domain, linking antibody response to RBD with neutralizing potential. Detection of IgG antibodies, rather than IgM or total antibodies, against RBD is likely to play a larger role in understanding antibody-mediated protection and vaccine response. Here we describe a rapid and stable RBD-based IgG ELISA test obtained through extensive optimization of the assay components and conditions. The test showed a specificity of 99.79% (95% CI: 98.82-99.99%) in a panel of pre-pandemic samples (n = 470) from different groups, i.e., pregnancy, fever, HCV, HBV, and autoantibodies positive. Test sensitivity was evaluated using sera from SARS-CoV-2 RT-PCR positive individuals (n = 312) and found to be 53.33% (95% CI: 37.87-68.34%), 80.47% (95% CI: 72.53-86.94%), and 88.24% (95% CI: 82.05-92.88%) in panel 1 (days 0-13), panel 2 (days 14-20) and panel 3 (days 21-27), respectively. Higher sensitivity was achieved in symptomatic individuals and reached 92.14% (95% CI: 86.38-96.01%) for panel 3. Our test, with a shorter runtime, showed higher sensitivity than parallelly tested commercial ELISAs for SARS-CoV-2-IgG, i.e., Euroimmun and Zydus, even when equivocal results in the commercial ELISAs were considered positive. None of the tests, which are using different antigens, could detect anti-SARS-CoV-2 IgGs in 10.5% RT-PCR positive individuals by the fourth week, suggesting the lack of IgG response.
Keywords: COVID-19; ELISA; RBD; SARS-CoV-2; SARS-CoV-2 IgG antibodies; diagnostics; receptor binding domain.
Copyright © 2021 Mehdi, Chattopadhyay, Thiruvengadam, Yadav, Kumar, Sinha, Goswami, Kshetrapal, Wadhwa, Chandramouli Natchu, Sopory, Koundinya Desiraju, Pandey, Das, Verma, Sharma, Sharma, Bhartia, Gosain, Lodha, Lamminmäki, Shrivastava, Bhatnagar and Batra.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Burbelo P. D., Riedo F. X., Morishima C., Rawlings S., Smith D., Das S., et al. (2020). Sensitivity in detection of antibodies to nucleocapsid and spike proteins of severe acute respiratory syndrome coronavirus 2 in patients with coronavirus disease 2019. J. Infect. Dis. 222 206–213. 10.1093/infdis/jiaa273 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous