

Prechemoradiotherapy Systemic Inflammation Response Index Stratifies Stage IIIB/C Non-Small-Cell Lung Cancer Patients into Three Prognostic Groups: A Propensity Score-Matching Analysis
- PMID: 33552158
- PMCID: PMC7847338
- DOI: 10.1155/2021/6688138
Prechemoradiotherapy Systemic Inflammation Response Index Stratifies Stage IIIB/C Non-Small-Cell Lung Cancer Patients into Three Prognostic Groups: A Propensity Score-Matching Analysis
Abstract
Purpose: We explored the prognostic influence of the systemic inflammation response index (SIRI) on the survival outcomes of stage IIIB/C non-small-cell lung cancer (NSCLC) patients who underwent concurrent chemoradiotherapy.
Methods: Present propensity score-matching (PSM) analysis comprised 876 stage IIIB/C NSCLC patients who received 1-3 cycles of platinum-based doublets concurrent with thoracic radiotherapy from 2007 to 2017. The primary and secondary objectives were the relationships between the SIRI values and overall (OS) and progression-free survival, respectively. Propensity scores were calculated for SIRI groups to adjust for confounders and to facilitate well-balanced comparability between the SIRI groups by creating 1 : 1 matched study groups.
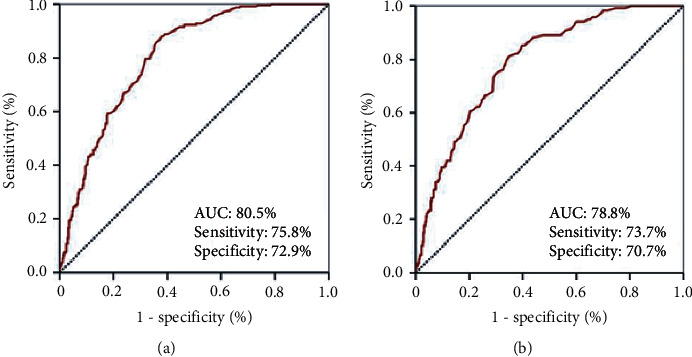
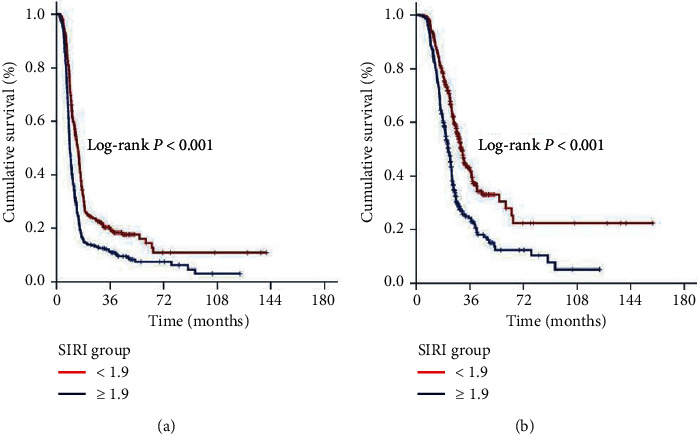
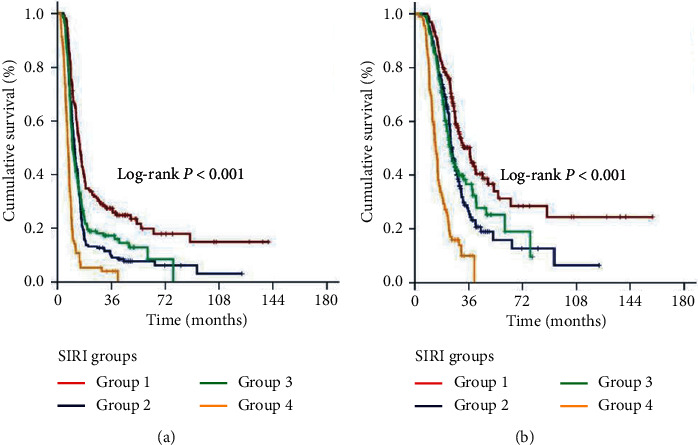
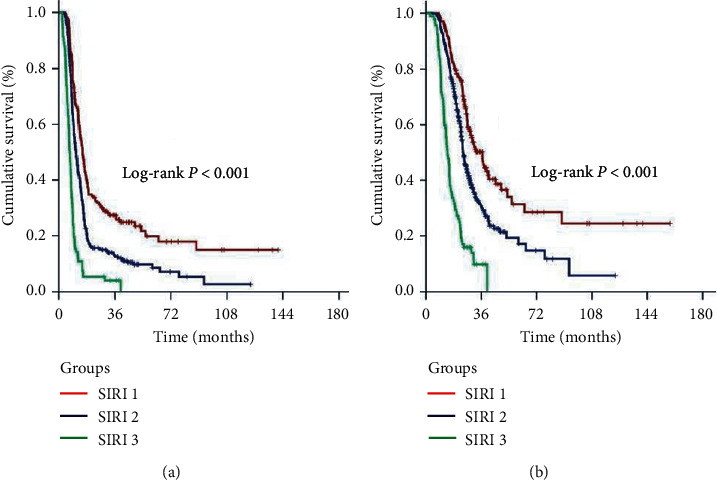
Results: The receiver operating characteristic curve analysis identified an optimal SIRI cutoff at 1.9 for OS (AUC: 78.8%; sensitivity: 73.7%; specificity: 70.7%) and PFS (AUC: 80.5%; sensitivity: 75.8%; specificity: 72.9%) and we grouped the patients into two PSM cohorts: SIRI < 1.9 (N = 304) and SIRI ≥ 1.9 (N = 304), respectively. The SIRI ≥ 1.9 cohort had significantly worse median OS (P < 0.001) and PFS (P < 0.001) than their SIRI < 1.9 companions. The further combination of SIRI with disease stage exhibited that the SIRI-1 (IIIB and SIRI < 1.9) and SIRI-3 (IIIC and SIRI ≥ 1.9) cohorts had the best and worst outcomes, respectively, with SIRI-2 cohort (IIIB and SIRI ≥ 1.9 or IIIC and SIRI < 1.9) being remained in between (P < 0.001 for OS and PFS, separately). In multivariate analysis, the two- and three-laddered stratifications per the 1.9 cutoffs and SIRI groups retained their independent significance, individually.
Conclusions: The SIRI ≥ 1.9 independently prognosticated significantly worse OS and PFS results and plated the stage IIIB/C patients into three fundamentally distinct prognostic groups.
Copyright © 2021 Erkan Topkan et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
-
- Furuse K., Fukuoka M., Kawahara M., et al. Phase III study of concurrent versus sequential thoracic radiotherapy in combination with mitomycin, vindesine, and cisplatin in unresectable stage III non-small-cell lung cancer. Journal of Clinical Oncology. 1999;17(9):p. 2692. doi: 10.1200/jco.1999.17.9.2692. - DOI - PubMed
-
- Bradley J. D., Paulus R., Komaki R., et al. Standard-dose versus high-dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non-small-cell lung cancer (RTOG 0617): a randomised, two-by-two factorial phase 3 study. The Lancet Oncology. 2015;16(2):187–199. doi: 10.1016/s1470-2045(14)71207-0. - DOI - PMC - PubMed
-
- Crohns M., Saarelainen S., Laine S., Poussa T., Alho H., Kellokumpu-Lehtinen P. Cytokines in bronchoalveolar lavage fluid and serum of lung cancer patients during radiotherapy-association of interleukin-8 and VEGF with survival. Cytokine. 2010;50(1):30–36. doi: 10.1016/j.cyto.2009.11.017. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
