

Short-Term Variations in Neutrophil-to-Lymphocyte and Urea-to-Creatinine Ratios Anticipate Intensive Care Unit Admission of COVID-19 Patients in the Emergency Department
- PMID: 33553217
- PMCID: PMC7854700
- DOI: 10.3389/fmed.2020.625176
Short-Term Variations in Neutrophil-to-Lymphocyte and Urea-to-Creatinine Ratios Anticipate Intensive Care Unit Admission of COVID-19 Patients in the Emergency Department
Abstract
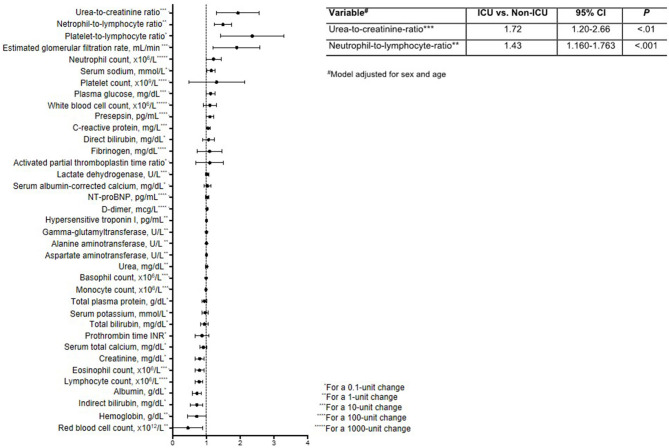
Background: Timely assessment of COVID-19 severity is crucial for the rapid provision of appropriate treatments. Definitive criteria for the early identification of severe COVID-19 cases that require intensive care unit admission are lacking. Methods: This was a single-center, retrospective case-control study of 95 consecutive adults admitted to the intensive care unit (cases) or a medical ward (controls) for laboratory-confirmed COVID-19. Clinical data were collected and changes in laboratory test results were calculated between presentation at the emergency department and admission. Univariate and multivariable logistic regression was performed to calculate odds ratios for intensive care unit admission according to changes in laboratory variables. Results: Of the 95 adults with COVID-19, 25 were admitted to intensive care and 70 to a medical ward after a median 6 h stay in the emergency department. During this interval, neutrophil counts increased in cases and decreased in controls (median, 934 vs. -295 × 106/L; P = 0.006), while lymphocyte counts decreased in cases and increased in controls (median, -184 vs. 109 × 106/L; P < 0.001). In cases, the neutrophil-to-lymphocyte ratio increased 6-fold and the urea-to-creatinine ratio increased 20-fold during the emergency department stay, but these ratios did not change in controls (P < 0.001 for both comparisons). By multivariable logistic regression, short-term increases in the neutrophil-to-lymphocyte ratio (OR = 1.43; 95% CI, 1.16-1.76) and urea-to-creatinine ratio (OR = 1.72; 95% CI, 1.20-2.66) were independent predictors of intensive care unit admission. Conclusion: Short-time changes in neutrophil-to-lymphocyte ratio and urea-to-creatinine ratio emerged as stand-alone parameters able to identify patients with aggressive disease at an early stage.
Keywords: COVID-19; disease severity; intensive care unit; neutrophil-to-lymphocyte ratio; urea-to-creatinine ratio.
Copyright © 2021 Solimando, Susca, Borrelli, Prete, Lauletta, Pappagallo, Buono, Inglese, Forina, Bochicchio, Capobianco, Carrieri, Cicco, Leone, Silvestris, Saracino, Ria, Procacci, Migliore, Vacca and Racanelli.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
LinkOut - more resources
Full Text Sources
Other Literature Sources