

A Machine-Learning Approach for Dynamic Prediction of Sepsis-Induced Coagulopathy in Critically Ill Patients With Sepsis
- PMID: 33553224
- PMCID: PMC7859637
- DOI: 10.3389/fmed.2020.637434
A Machine-Learning Approach for Dynamic Prediction of Sepsis-Induced Coagulopathy in Critically Ill Patients With Sepsis
Abstract
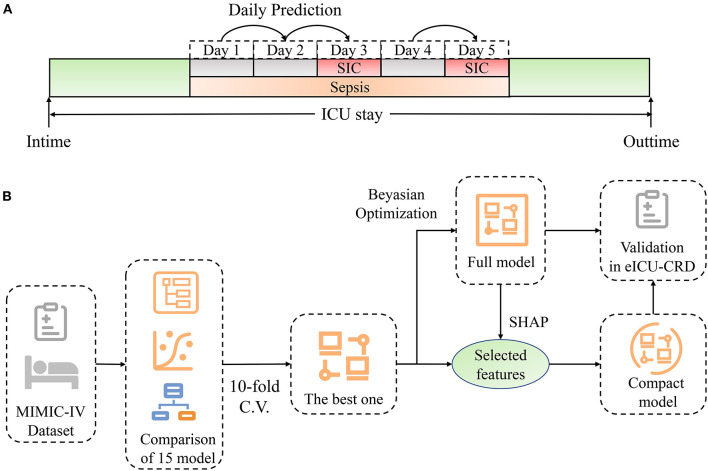
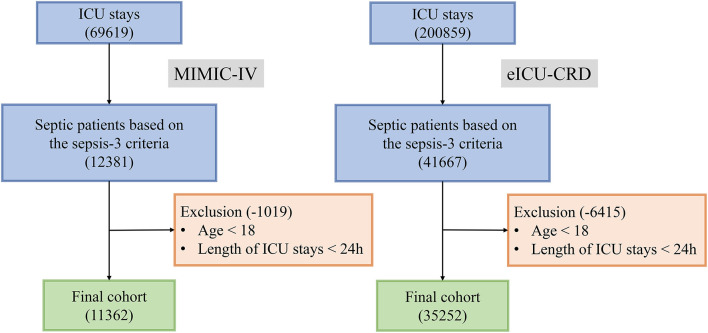
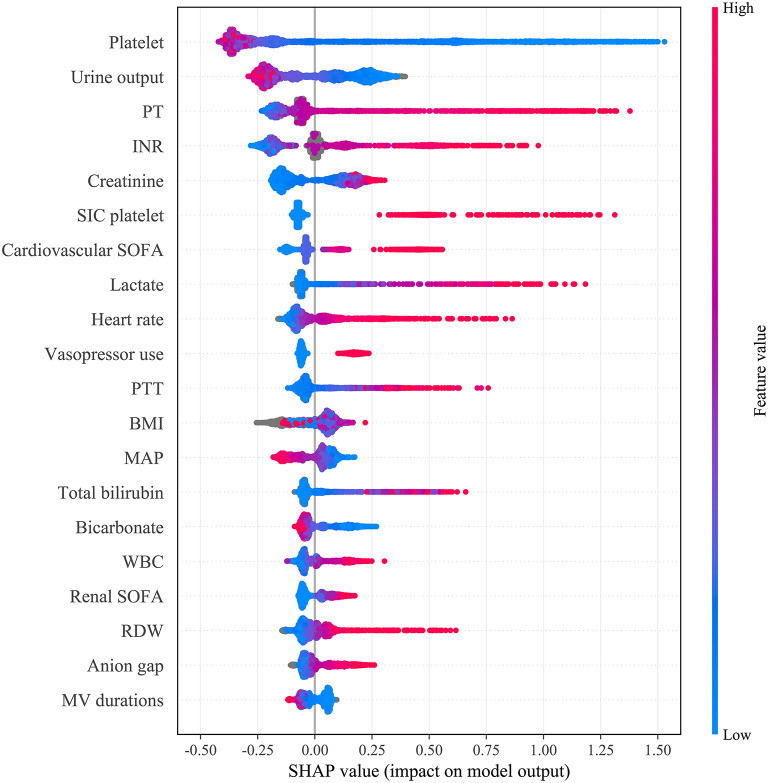
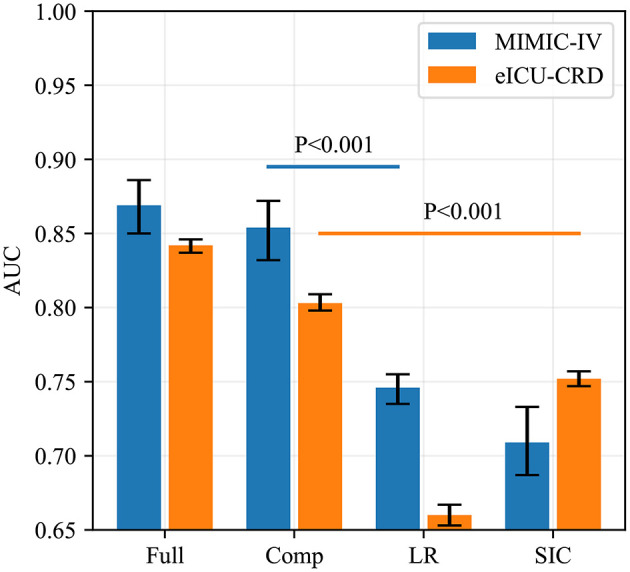
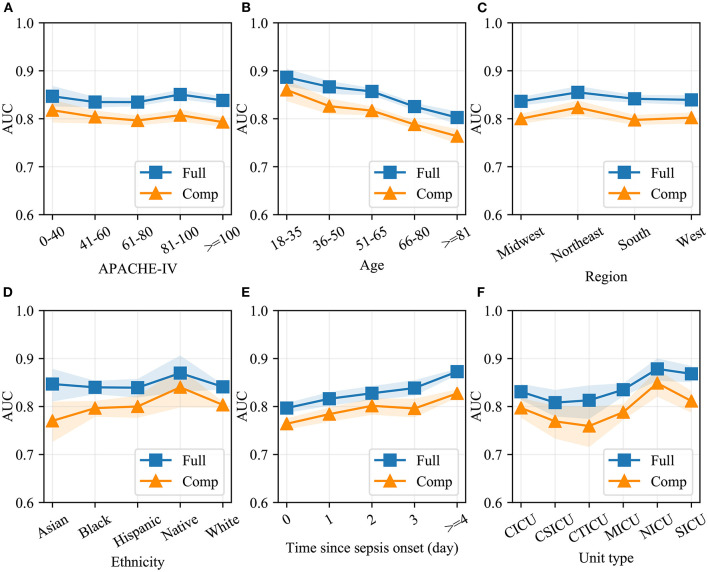
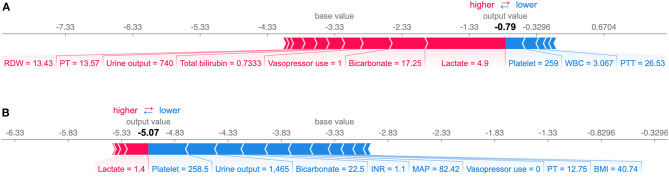
Background: Sepsis-induced coagulopathy (SIC) denotes an increased mortality rate and poorer prognosis in septic patients. Objectives: Our study aimed to develop and validate machine-learning models to dynamically predict the risk of SIC in critically ill patients with sepsis. Methods: Machine-learning models were developed and validated based on two public databases named Medical Information Mart for Intensive Care (MIMIC)-IV and the eICU Collaborative Research Database (eICU-CRD). Dynamic prediction of SIC involved an evaluation of the risk of SIC each day after the diagnosis of sepsis using 15 predictive models. The best model was selected based on its accuracy and area under the receiver operating characteristic curve (AUC), followed by fine-grained hyperparameter adjustment using the Bayesian Optimization Algorithm. A compact model was developed, based on 15 features selected according to their importance and clinical availability. These two models were compared with Logistic Regression and SIC scores in terms of SIC prediction. Results: Of 11,362 patients in MIMIC-IV included in the final cohort, a total of 6,744 (59%) patients developed SIC during sepsis. The model named Categorical Boosting (CatBoost) had the greatest AUC in our study (0.869; 95% CI: 0.850-0.886). Coagulation profile and renal function indicators were the most important features for predicting SIC. A compact model was developed with an AUC of 0.854 (95% CI: 0.832-0.872), while the AUCs of Logistic Regression and SIC scores were 0.746 (95% CI: 0.735-0.755) and 0.709 (95% CI: 0.687-0.733), respectively. A cohort of 35,252 septic patients in eICU-CRD was analyzed. The AUCs of the full and the compact models in the external validation were 0.842 (95% CI: 0.837-0.846) and 0.803 (95% CI: 0.798-0.809), respectively, which were still larger than those of Logistic Regression (0.660; 95% CI: 0.653-0.667) and SIC scores (0.752; 95% CI: 0.747-0.757). Prediction results were illustrated by SHapley Additive exPlanations (SHAP) values, which made our models clinically interpretable. Conclusions: We developed two models which were able to dynamically predict the risk of SIC in septic patients better than conventional Logistic Regression and SIC scores.
Keywords: Logistic Regression; dynamic prediction; external validation; machine learning; model interpretation; sepsis-induced coagulopathy.
Copyright © 2021 Zhao, Liu, Luo, Luo, Wang, Zhang, Gui, Tu and Luo.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Interpretable machine learning model for early prediction of 28-day mortality in ICU patients with sepsis-induced coagulopathy: development and validation.Eur J Med Res. 2024 Jan 3;29(1):14. doi: 10.1186/s40001-023-01593-7. Eur J Med Res. 2024. PMID: 38172962 Free PMC article.
-
Interpretable machine learning for 28-day all-cause in-hospital mortality prediction in critically ill patients with heart failure combined with hypertension: A retrospective cohort study based on medical information mart for intensive care database-IV and eICU databases.Front Cardiovasc Med. 2022 Oct 12;9:994359. doi: 10.3389/fcvm.2022.994359. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36312291 Free PMC article.
-
Identification and Validation of an Explainable Prediction Model of Sepsis in Patients With Intracerebral Hemorrhage: Multicenter Retrospective Study.J Med Internet Res. 2025 Apr 28;27:e71413. doi: 10.2196/71413. J Med Internet Res. 2025. PMID: 40293793 Free PMC article.
-
Management Strategies in Septic Coagulopathy: A Review of the Current Literature.Healthcare (Basel). 2023 Jan 12;11(2):227. doi: 10.3390/healthcare11020227. Healthcare (Basel). 2023. PMID: 36673595 Free PMC article. Review.
-
Machine Learning Models in Sepsis Outcome Prediction for ICU Patients: Integrating Routine Laboratory Tests-A Systematic Review.Biomedicines. 2024 Dec 19;12(12):2892. doi: 10.3390/biomedicines12122892. Biomedicines. 2024. PMID: 39767798 Free PMC article. Review.
Cited by
-
Predicting acute kidney injury risk in acute myocardial infarction patients: An artificial intelligence model using medical information mart for intensive care databases.Front Cardiovasc Med. 2022 Sep 7;9:964894. doi: 10.3389/fcvm.2022.964894. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36158815 Free PMC article.
-
A Machine Learning Approach for the Prediction of Traumatic Brain Injury Induced Coagulopathy.Front Med (Lausanne). 2021 Dec 10;8:792689. doi: 10.3389/fmed.2021.792689. eCollection 2021. Front Med (Lausanne). 2021. PMID: 34957161 Free PMC article.
-
Drug-induced coagulopathies: a real-world pharmacovigilance study using the FDA adverse event reporting system.Front Pharmacol. 2024 Dec 18;15:1486422. doi: 10.3389/fphar.2024.1486422. eCollection 2024. Front Pharmacol. 2024. PMID: 39744131 Free PMC article.
-
A Retrospective Cohort Study: Predicting 90-Day Mortality for ICU Trauma Patients with a Machine Learning Algorithm Using XGBoost Using MIMIC-III Database.J Multidiscip Healthc. 2023 Sep 6;16:2625-2640. doi: 10.2147/JMDH.S416943. eCollection 2023. J Multidiscip Healthc. 2023. PMID: 37701177 Free PMC article.
-
Association of serum phosphate and changes in serum phosphate with 28-day mortality in septic shock from MIMIC-IV database.Sci Rep. 2023 Dec 10;13(1):21869. doi: 10.1038/s41598-023-49170-6. Sci Rep. 2023. PMID: 38072848 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources