

Late response to rosuvastatin and statin-related myalgia due to SLCO1B1, SLCO1B3, ABCB11, and CYP3A5 variants in a patient with Familial Hypercholesterolemia: a case report
- PMID: 33553369
- PMCID: PMC7859822
- DOI: 10.21037/atm-20-5540
Late response to rosuvastatin and statin-related myalgia due to SLCO1B1, SLCO1B3, ABCB11, and CYP3A5 variants in a patient with Familial Hypercholesterolemia: a case report
Abstract
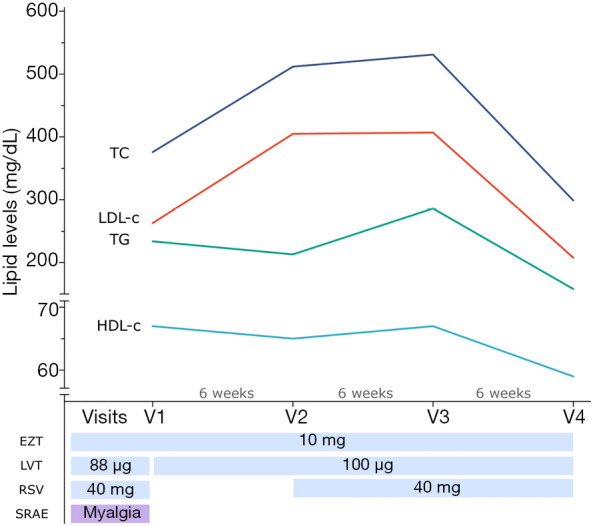
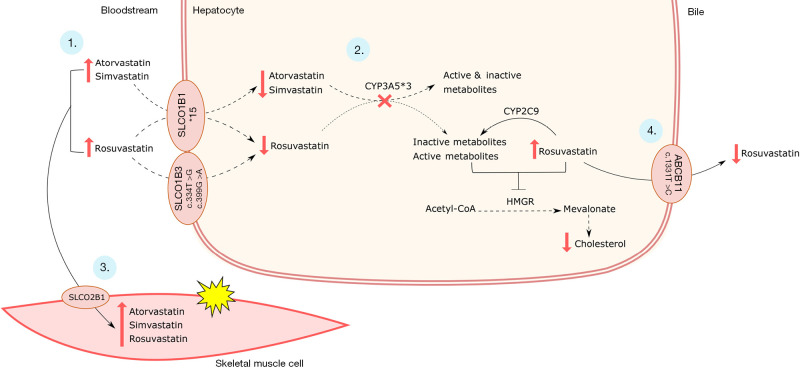
Statins are the most widely used cholesterol-lowering drugs for cardiovascular diseases prevention. However, some patients are refractory to treatment, whereas others experience statin-related adverse events (SRAE). It has been increasingly important to identify pharmacogenetic biomarkers for predicting statin response and adverse events. This case report describes a female patient with familial hypercholesterolemia (FH) who showed late response to rosuvastatin and experienced myalgia on statin treatment. In the first visit (V1), the patient reported myalgia to rosuvastatin 40 mg, which was interrupted for a 6-week wash-out period. In V2, rosuvastatin 20 mg was reintroduced, but her lipid profile did not show any changes after 6 weeks (V3) (LDL-c: 402 vs. 407 mg/dL). Her lipid profile markedly improved after 12 weeks of treatment (V4) (LDL-c: 208 mg/dL), suggesting a late rosuvastatin response. Her adherence to treatment was similar in V1 and V3 and no drug interactions were detected. Pharmacogenetic analysis revealed that the patient carries low-activity variants in SLCO1B1*1B and*5, SLCO1B3 (rs4149117 and rs7311358), and ABCB11 rs2287622, and the non-functional variant in CYP3A5*3. The combined effect of variants in pharmacokinetics-related genes may have contributed to the late response to rosuvastatin and statin-related myalgia. Therefore, they should be considered when assessing a patient's response to statin treatment. To the best of our knowledge, this is the first report of a pharmacogenetic analysis on a case of late rosuvastatin response.
Keywords: Pharmacogenetics; familial hypercholesterolemia (FH); myalgia; precision medicine; statins.
2021 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/atm-20-5540). The authors have no conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous