

Long-term outcomes of perianal fistulizing Crohn's disease in the biologic era
- PMID: 33553661
- PMCID: PMC7857282
- DOI: 10.1002/jgh3.12475
Long-term outcomes of perianal fistulizing Crohn's disease in the biologic era
Abstract
Background and aim: While the advent of biologic therapy has led to improved outcomes in perianal fistulizing Crohn's disease (pfCD), loss of response is common. Previous studies suggest that patients who achieve radiological healing (with healing of underlying tracts on magnetic resonance imaging [MRI]) have a longer duration of response. The aim of this study was to characterize MRI outcomes of pfCD at a specialist inflammatory bowel disease (IBD) unit and compare the long-term clinical outcomes between patients achieving MRI and clinical healing.
Methods: A retrospective analysis of perianal fistulizing Crohn's patients treated at one specialist IBD unit was performed. Records were reviewed for patient demographics, disease history, clinical assessments, investigation results, and disease flares. Clinical remission was defined as closure of all baseline fistula openings. Radiological healing was defined as the absence of any T2-hyperintense sinuses, tracts, or collections. The primary end-point was rate of MRI healing. The secondary outcome was defined as flare-free period (time between clinical or radiological healing and patients' first signs/symptoms requiring therapy escalation).
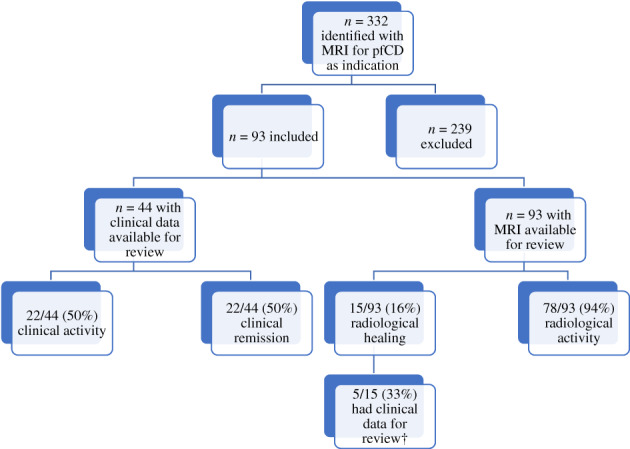
Results: A total of 93 patients were included, with a median follow-up of 4.8 years (interquartile range, 2.4-6 years). Of 44 patients, 22 (50%) achieved clinical remission, while 15 of 93 (16%) achieved radiological healing. Of 22 patients, 10 (45%) with clinical remission had a subsequent disease flare (median time of 7 months) compared with 3 of 15 (20%) patients with MRI healing (median time of 3.6 years). Radiological healing was associated with a significantly longer flare-free period (P = 0.01).
Conclusion: Radiological healing occurs less commonly but represents a deeper form of healing, associated with improved long-term clinical outcomes.
Keywords: Crohn's disease; biological therapy; magnetic resonance imaging; perianal fistula; tumor necrosis factor‐alpha.
© 2020 The Authors. JGH Open: An open access journal of gastroenterology and hepatology published by Journal of Gastroenterology and Hepatology Foundation and John Wiley & Sons Australia, Ltd.
Figures
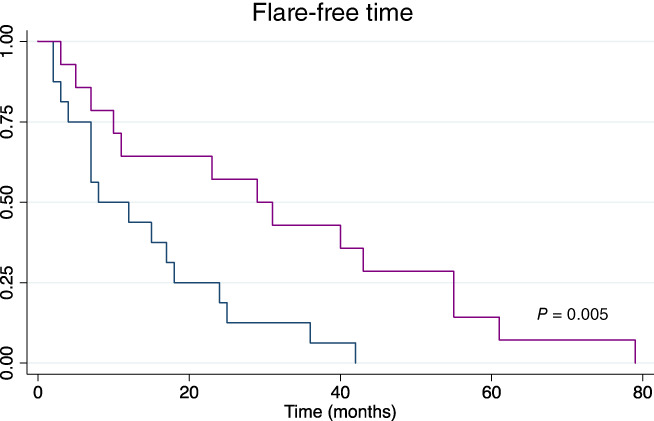
 ), Clinical remission; (
), Clinical remission; ( ), radiological healing.
), radiological healing.References
-
- Ng SC, Plamondon S, Gupta A, Burling D, Kamm MA. Prospective assessment of the effect on quality of life of anti‐tumour necrosis factor therapy for perineal Crohn's fistulas. Aliment. Pharmacol. Ther. 2009; 30: 757–66. - PubMed
-
- Sandborn WJ, Fazio VW, Feagan BG, Hanauer SB. AGA technical review on perianal Crohn's disease. Gastroenterology. 2003; 125: 1508–30. - PubMed
-
- Yassin NA, Askari A, Warusavitarne J et al Systematic review: the combined surgical and medical treatment of fistulising perianal Crohn's disease. Aliment. Pharmacol. Ther. 2014; 40: 741–9. - PubMed
-
- Lichenstein G, Yan S, Bala M, Blank M, Sands BE. Infliximab maintenance treatment reduces hospitalizations, surgeries, and procedures in fistulizing Crohn's disease. Gastroenterology. 2005; 128: 862–9. - PubMed
LinkOut - more resources
Full Text Sources
