

Chemoradiation induced multiple sclerosis-like demyelination
- PMID: 33553701
- PMCID: PMC7851181
- DOI: 10.1016/j.ensci.2021.100315
Chemoradiation induced multiple sclerosis-like demyelination
Abstract
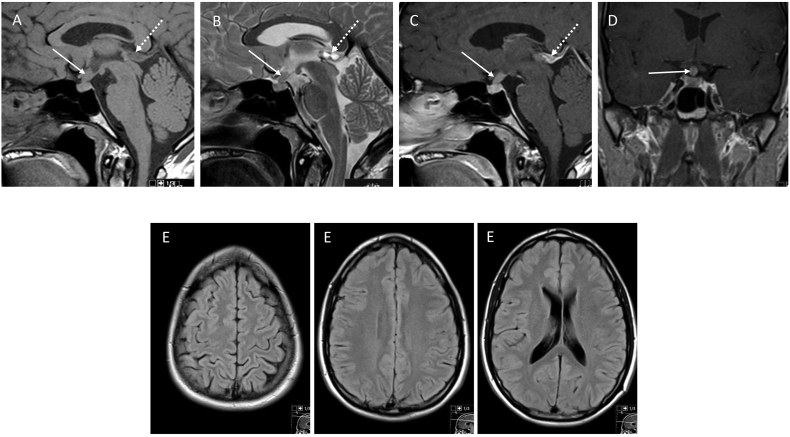
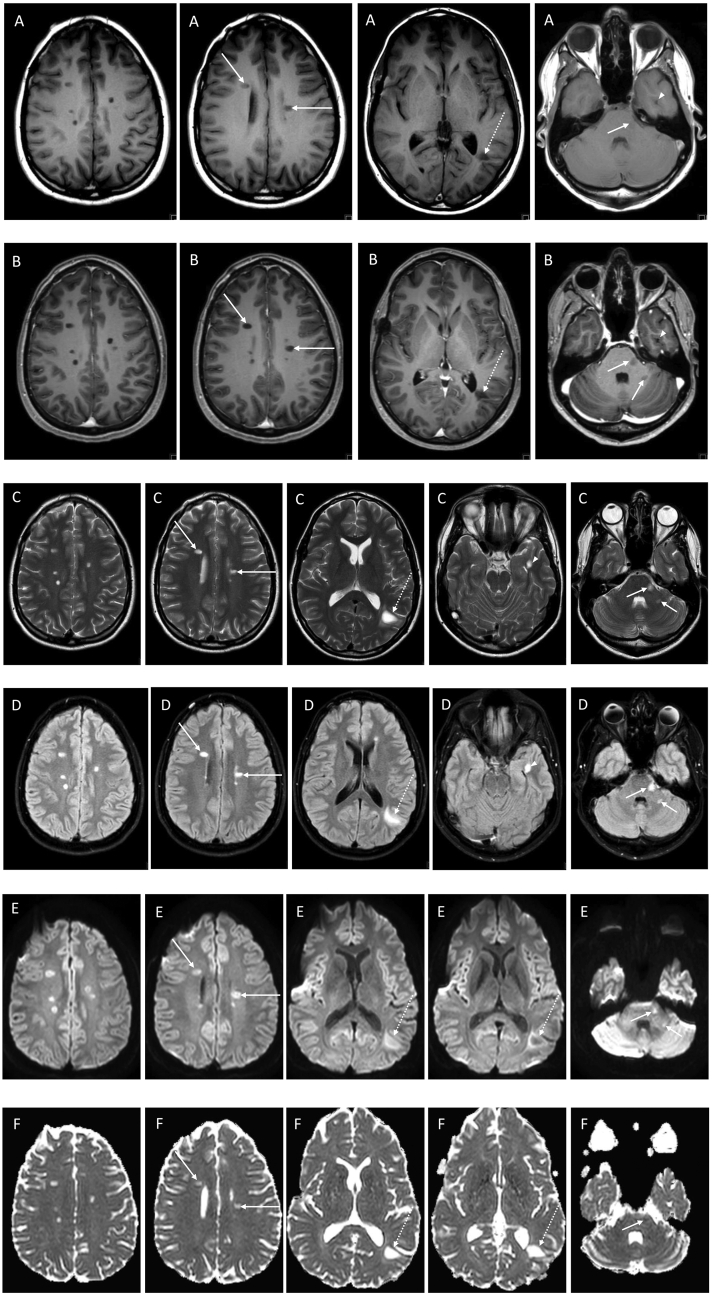
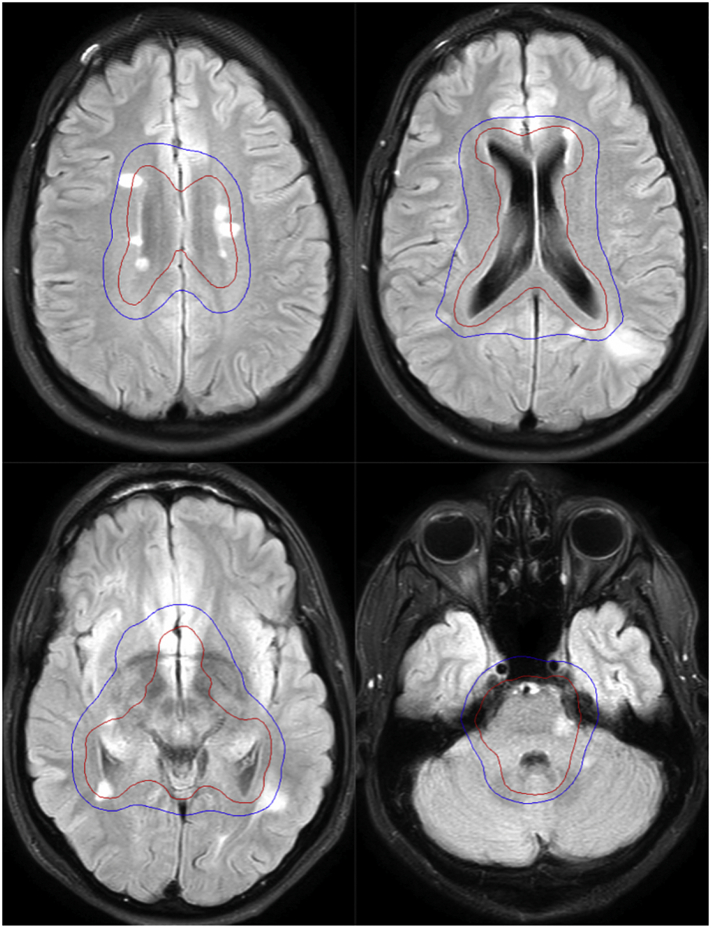
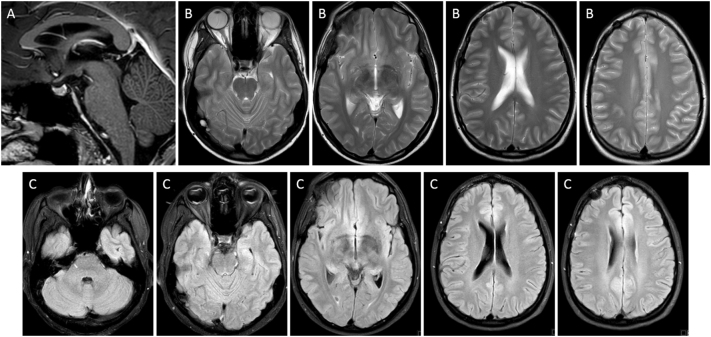
We report the case of a 28-year-old man, diagnosed with a non-secreting, non-metastatic suprasellar germinoma treated with chemoradiation who developed, four months after completion of radiation therapy, multiple discrete demyelinating lesions mimicking multiple sclerosis (MS). The patient had no previous diagnosis of MS and the neuroimaging studies performed both at the time of diagnosis and after chemotherapy, pre-irradiation, showed no evidence of white matter lesions. He remained asymptomatic, with no focal neurological deficits. Biochemical analysis of the CSF was positive for the intrathecal synthesis of IgG with oligoclonal bands. Follow-up MRI six months later showed a spontaneous decrease in lesion size and resolution of associated inflammatory signs, with lesions remaining stable in number. We discuss the potential origin of these white matter lesions, which may correspond to MS-like late-delayed demyelination secondary to chemoradiation therapy, in a previously predisposed patient.
Keywords: Chemorradiation-induced demyelination; Chemorradiation-induced neurotoxicity; MRI; Multiple sclerosis-like demyelination; Neuro-oncology.
© 2021 The Authors.
Conflict of interest statement
None.
Figures
References
-
- Seigers R., Schagen S.B., Coppens C.M., van der Most P.J., van Dam F.S., Koolhaas J.M., Buwalda B. Methotrexate decreases hippocampal cell proliferation and induces memory deficits in rats. Behav. Brain Res. 2009;201:279–284. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
