

Carbon nanomaterials for cardiovascular theranostics: Promises and challenges
- PMID: 33553814
- PMCID: PMC7829079
- DOI: 10.1016/j.bioactmat.2020.12.030
Carbon nanomaterials for cardiovascular theranostics: Promises and challenges
Abstract
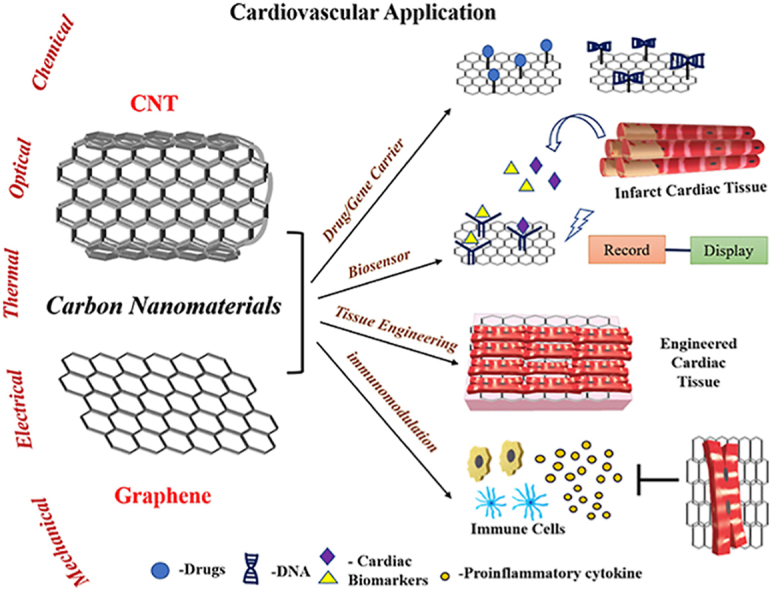
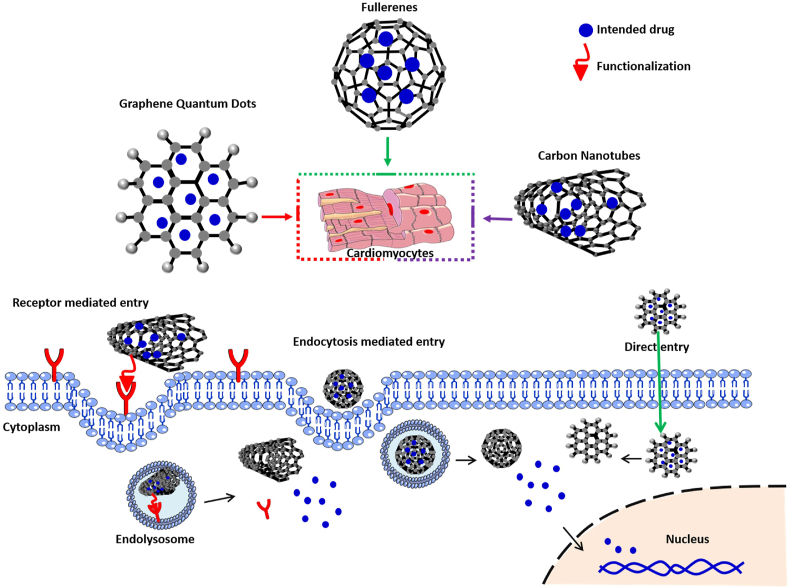
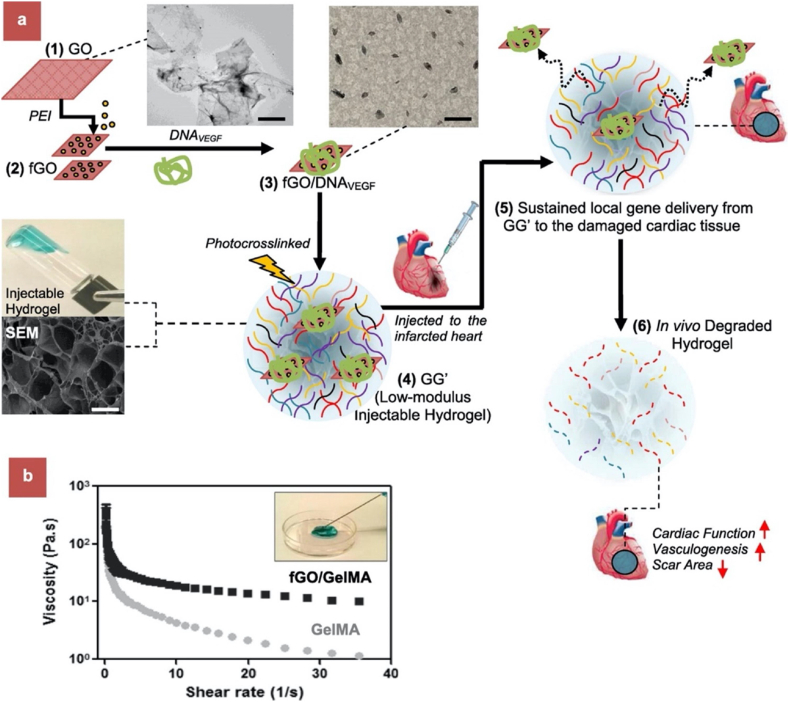
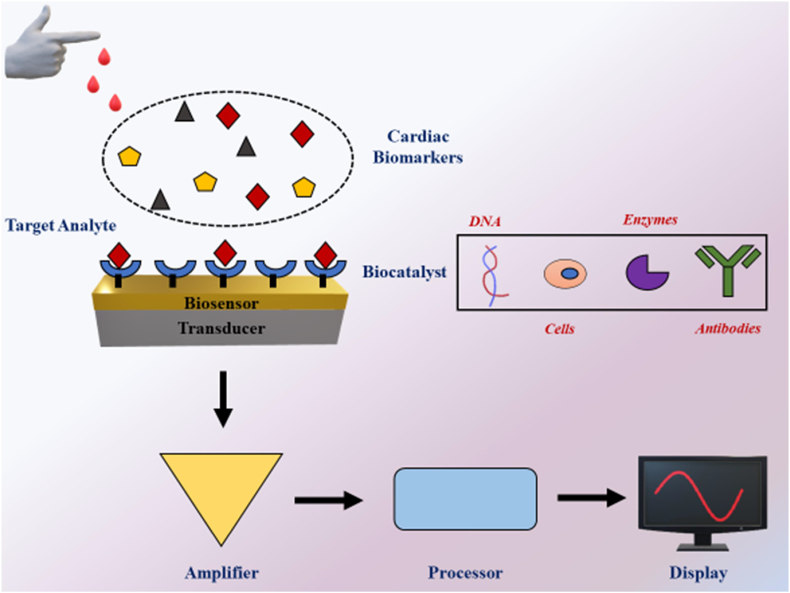
Cardiovascular diseases (CVDs) are the leading cause of death worldwide. Heart attack and stroke cause irreversible tissue damage. The currently available treatment options are limited to "damage-control" rather than tissue repair. The recent advances in nanomaterials have offered novel approaches to restore tissue function after injury. In particular, carbon nanomaterials (CNMs) have shown significant promise to bridge the gap in clinical translation of biomaterial based therapies. This family of carbon allotropes (including graphenes, carbon nanotubes and fullerenes) have unique physiochemical properties, including exceptional mechanical strength, electrical conductivity, chemical behaviour, thermal stability and optical properties. These intrinsic properties make CNMs ideal materials for use in cardiovascular theranostics. This review is focused on recent efforts in the diagnosis and treatment of heart diseases using graphenes and carbon nanotubes. The first section introduces currently available derivatives of graphenes and carbon nanotubes and discusses some of the key characteristics of these materials. The second section covers their application in drug delivery, biosensors, tissue engineering and immunomodulation with a focus on cardiovascular applications. The final section discusses current shortcomings and limitations of CNMs in cardiovascular applications and reviews ongoing efforts to address these concerns and to bring CNMs from bench to bedside.
Keywords: Biosensors; Carbon nanomaterials; Cardiac tissue engineering; Cardiovascular disease; Drug delivery; Immunomodulation.
© 2021 [The Author/The Authors].
Conflict of interest statement
Authors declare no conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
