

Nonalcoholic Fatty Liver Disease Screening in Type 2 Diabetes Mellitus Patients in the Primary Care Setting
- PMID: 33553966
- PMCID: PMC7850314
- DOI: 10.1002/hep4.1618
Nonalcoholic Fatty Liver Disease Screening in Type 2 Diabetes Mellitus Patients in the Primary Care Setting
Abstract
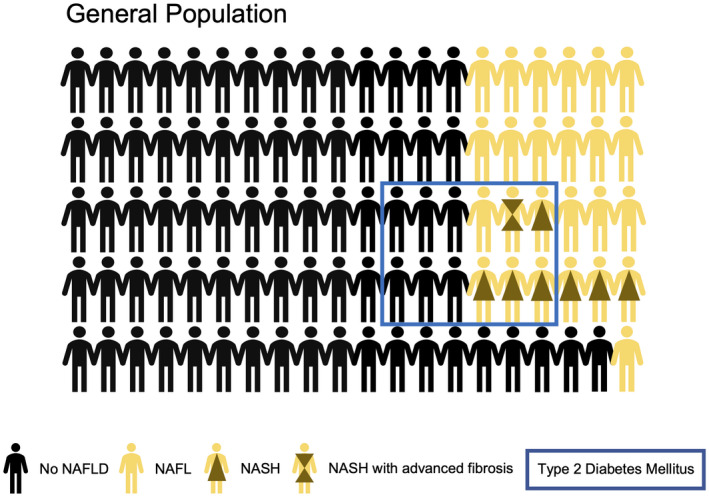
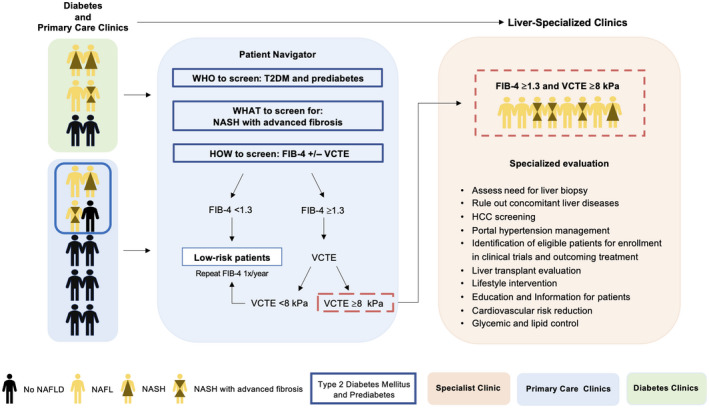
Nonalcoholic fatty liver disease (NAFLD) is a major public health problem worldwide and the most common chronic liver disease. NAFLD currently affects approximately one in every four people in the United States, and its global burden is expected to rise in the next decades. Despite being a prevalent disease in the general population, only a minority of patients with NAFLD will develop nonalcoholic steatohepatitis (NASH) with advanced liver fibrosis (stage 3-4 fibrosis) and liver-related complications. Certain populations, such as patients with type 2 diabetes mellitus (T2DM), are recognized to be at the highest risk for developing NASH and advanced fibrosis. Both the American Diabetes Association and the European Association for the Study of Diabetes recommend screening of all T2DM for NAFLD. Incorporating a simple noninvasive algorithm into the existing diabetic care checklists in the primary care practice or diabetologist's office would efficiently identify patients at high risk who should be referred to specialists. The proposed algorithm involves a first-step annual fibrosis-4 score (FIB-4) followed by vibration-controlled transient elastography (VCTE) for those with indeterminate or high-risk score (FIB-4 ≥1.3). Patients at low-risk (FIB-4 <1.3 or VCTE <8 kPa) can be followed up by primary care providers for lifestyle changes and yearly calculation of FIB-4, while patients at high risk (FIB-4 ≥1.3 and VCTE ≥8 kPa) should be referred to a liver-specialized center. Conclusion: Patients with T2DM or prediabetes should be screened for NASH and advanced fibrosis. The proposed simple algorithm can be easily incorporated into the existing workflow in the primary care or diabetology clinic to identify patients at high risk for NASH and advanced fibrosis who should be referred to liver specialists.
© 2020 The Authors. Hepatology Communications published by Wiley Periodicals LLC on behalf of American Association for the Study of Liver Diseases.
Figures
References
-
- Younossi Z, Tacke F, Arrese M, Chander Sharma B, Mostafa I, Bugianesi E, et al. Global perspectives on nonalcoholic fatty liver disease and nonalcoholic steatohepatitis. Hepatology 2019;69:2672‐2682. - PubMed
-
- Cotter TG, Rinella M. Nonalcoholic fatty liver disease 2020: the state of the disease. Gastroenterology 2020;158:1851‐1864. - PubMed
-
- Younossi ZM, Stepanova M, Younossi Y, Golabi P, Mishra A, Rafiq N, et al. Epidemiology of chronic liver diseases in the USA in the past three decades. Gut 2020;69:564‐568. - PubMed
-
- Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease‐Meta‐analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016;64:73‐84. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
