

Reduced Clot Stability by Thromboelastography as a Potential Indicator of Procedure-Related Bleeding in Decompensated Cirrhosis
- PMID: 33553974
- PMCID: PMC7850311
- DOI: 10.1002/hep4.1641
Reduced Clot Stability by Thromboelastography as a Potential Indicator of Procedure-Related Bleeding in Decompensated Cirrhosis
Abstract
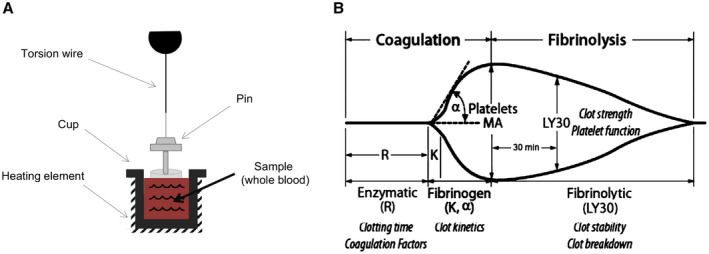
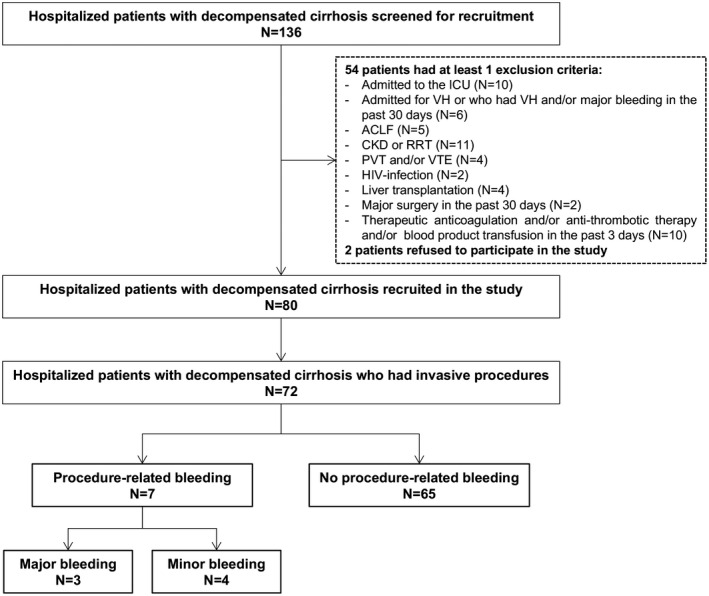
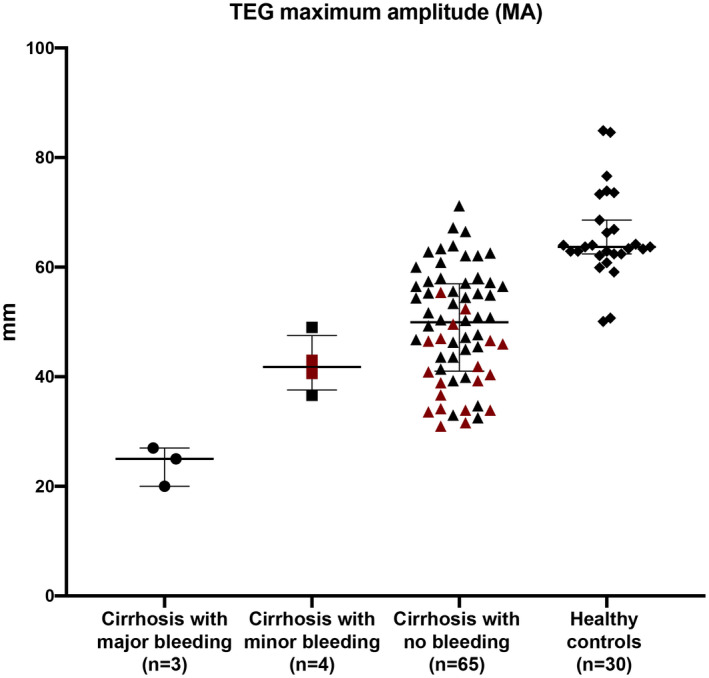
In patients with decompensated cirrhosis, procedure-related bleeding is a potentially lethal complication. Routine coagulation tests such as international normalized ratio and platelet count do not predict bleeding risk. We investigated whether thromboelastography (TEG) can identify patients with cirrhosis who are at risk of procedure-related bleeding. As a part of a prospective study on hemostasis in decompensated cirrhosis, patients had TEG performed on admission and were followed prospectively during hospitalization for the development of procedure-related bleeding. Eighty patients with cirrhosis were included. Among the 72 who had procedures performed, 7 had procedure-related bleeding, which was major in three cases (two following paracentesis and one following thoracentesis). Conventional coagulation tests were comparable between bleeding and nonbleeding patients, whereas TEG parameters of k-time (4.5 minutes vs. 2.2 minutes; P = 0.02), α-angle (34° vs. 59°; P = 0.003), and maximum amplitude (37 mm vs. 50 mm; P = 0.004) were significantly different (all indicative of hypocoagulability). TEG maximum amplitude (MA), a marker of overall clot stability, accurately discriminated between patients who had major, life-threatening bleeding (all with MA < 30 mm) and those who had mild or no bleeding (all with MA > 30 mm), whereas a platelet count < 50 × 109/L could not discriminate between bleeding (minor or major) and nonbleeding patients. Conclusion: In a prospective cohort of hospitalized patients with decompensated cirrhosis, TEG parameters associated with hypocoagulability appeared to predict procedure-related bleeding, particularly a TEG MA < 30 mm. If results are validated in a larger cohort, this could be a threshold to identify patients with decompensated cirrhosis at higher risk for procedure-related bleeding, in whom to consider preprocedural prophylaxis.
© 2020 The Authors. Hepatology Communications published by Wiley Periodicals LLC on behalf of the American Association for the Study of Liver Diseases.
Figures
References
-
- De Gottardi A, Thévenot T, Spahr L, Morard I, Bresson–Hadni S, Torres F, et al. Risk of complications after abdominal paracentesis in cirrhotic patients: a prospective study. Clin Gastroenterol Hepatol 2009;7:906‐909. - PubMed
-
- Mallory A, Schaefer JW. Complications of diagnostic paracentesis in patients with liver disease. JAMA 1978;239:628‐630. - PubMed
-
- Pache I, Bilodeau M. Severe haemorrhage following abdominal paracentesis for ascites in patients with liver disease. Aliment Pharmacol Ther 2005;21:525‐529. - PubMed
-
- Rowley MW, Agarwal S, Seetharam AB, Hirsch KS. Real‐time ultrasound‐guided paracentesis by radiologists: near zero risk of hemorrhage without correction of coagulopathy. J Vasc Interv Radiol 2019;30:259‐264. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
