

Longitudinal evaluation of risk factors and outcomes of blood stream infections due to Staphylococcu s species in persons with HIV: An observational cohort study
- PMID: 33554080
- PMCID: PMC7846664
- DOI: 10.1016/j.eclinm.2020.100675
Longitudinal evaluation of risk factors and outcomes of blood stream infections due to Staphylococcu s species in persons with HIV: An observational cohort study
Abstract
Background: Staphylococcal blood stream infections (SBSI) are a significant cause of morbidity and mortality, however there is little data on such infections in persons with HIV (PWH) in the combination antiretroviral therapy era, particularly when divided by species; methicillin-sensitive (MSSA) and methicillin-resistant Staphylococcus aureus (MRSA) and coagulase-negative Staphylococcus (CoNS).
Methods: Using linked longitudinal clinical and microbiologic databases, all cases of SBSI in PWH accessing care at Southern Alberta Clinic were identified and demographic features and outcomes characterized. We compared participants with SBSI to those with no SBSI and determined the 1-year all-cause mortality following SBSI and longitudinally over the study period.
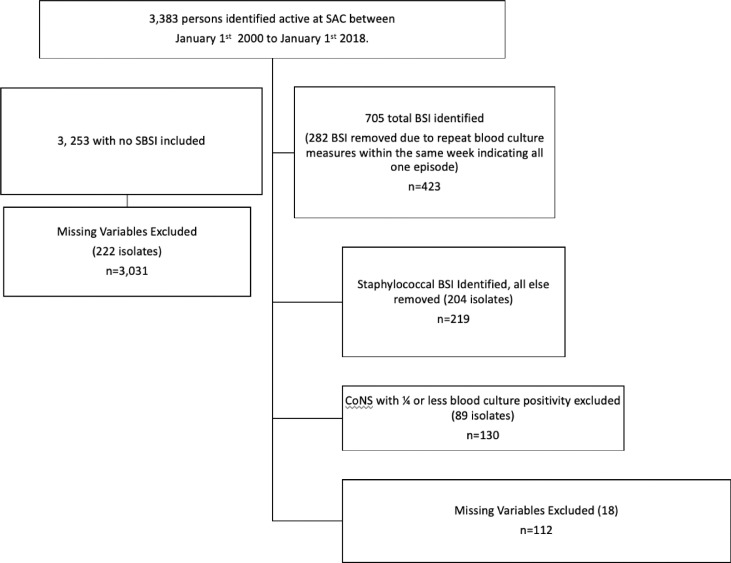
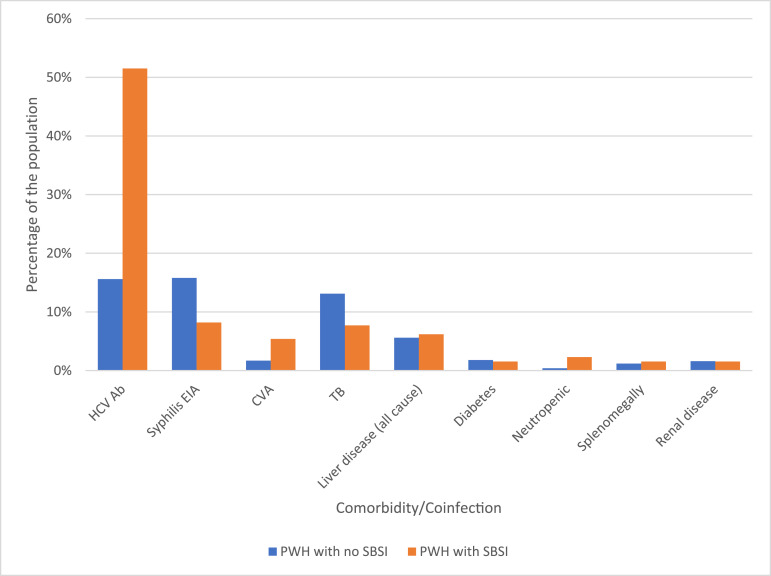
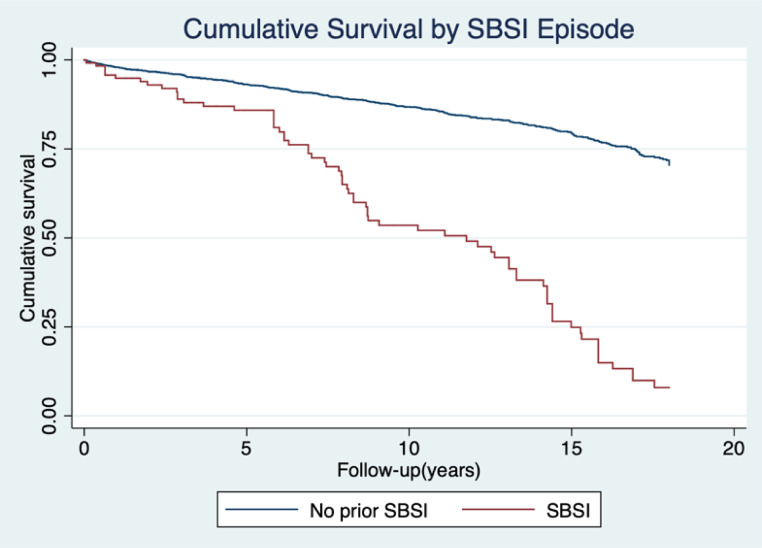
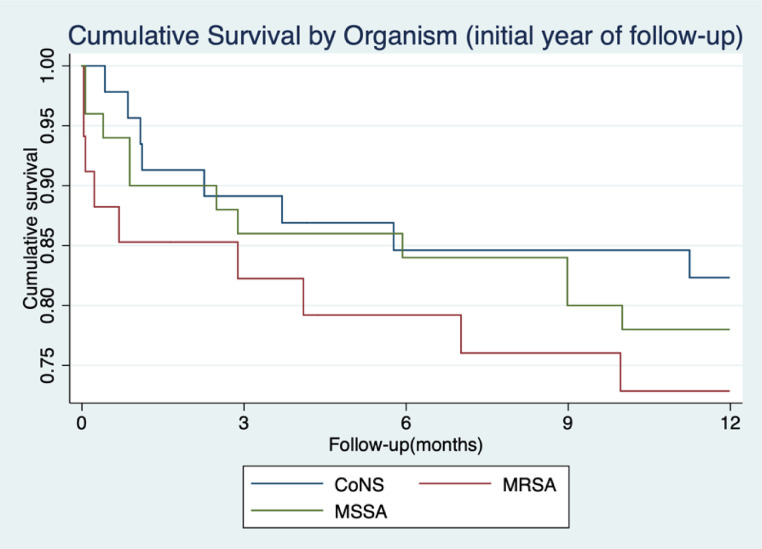
Findings: From 2000 to 2018, 130 SBSI occurred in 95 PWH over 21,526 patient-years follow-up. MSSA caused 38.4%, MRSA 26.1% and CoNS 35.3% of SBSI. Highest risks for SSBI were in Hepatitis C coinfection, low CD4 nadir, Indigenous/Metis ethnicity and in persons who use injection drugs (PWID). During follow-up, 423 deaths occurred in all PWH. Mortality rates for PWH with SBSI was 74.9/1000 patient-years (95% CI 59.2-94.9) compared with no SBSI 16.0/1000 patient-years (95% CI 14.4-17.7). The mortality Hazard Ratio was 2.61(95% CI 1.95-3.49, P= <0.001) for SBSI compared to no SBSI, following adjusting for confounding. Seventy deaths occurred in persons with SBSI with 40% in the first year. Higher 1-year mortality rates occurred in hospital-acquired infections.
Interpretation: Incidence rates of SBSI are high in PWH, with identified characteristics that further increase this risk. PWH who experience SBSI have a significant mortality risk within the first year of follow-up, however they also have greater long-term all-cause mortality compared to those with no SBSI. Further investigation is needed in PWH evaluating host, environment and pathogen differences that lead to differing rates of SBSI and mortality seen here.
Funding: No funding was received for this work.
Keywords: Bloodstream infections; Coagulase negative staphylococcus; HIV/AIDS; Outcomes; Staphylococcus aureus.
© 2020 The Authors.
Conflict of interest statement
MJ Gill has received honoraria as ad hoc member of national HIV advisory Boards to Merck, ViiV and Gilead. All other authors report no conflict.
Figures
Similar articles
-
Risk Factors and Outcomes of Bloodstream Infections Among People With Human Immunodeficiency Virus: A Longitudinal Cohort Study From 2000 to 2017.Open Forum Infect Dis. 2022 Aug 3;9(8):ofac318. doi: 10.1093/ofid/ofac318. eCollection 2022 Aug. Open Forum Infect Dis. 2022. PMID: 35937645 Free PMC article.
-
Trends in Hepatocellular Carcinoma Incidence and Risk Among Persons With HIV in the US and Canada, 1996-2015.JAMA Netw Open. 2021 Feb 1;4(2):e2037512. doi: 10.1001/jamanetworkopen.2020.37512. JAMA Netw Open. 2021. PMID: 33595662 Free PMC article.
-
A comparison of long-term outcomes after meticillin-resistant and meticillin-sensitive Staphylococcus aureus bacteraemia: an observational cohort study.Lancet Infect Dis. 2014 Oct;14(10):967-75. doi: 10.1016/S1473-3099(14)70876-X. Epub 2014 Aug 31. Lancet Infect Dis. 2014. PMID: 25185461
-
Methicillin-resistant Staphylococcus aureus (MRSA) infections among HIV-infected persons in the era of highly active antiretroviral therapy: a review of the literature.HIV Med. 2012 Jul;13(6):319-32. doi: 10.1111/j.1468-1293.2011.00978.x. Epub 2012 Jan 25. HIV Med. 2012. PMID: 22276696 Review.
-
A comparison of clinical virulence of nosocomially acquired methicillin-resistant and methicillin-sensitive Staphylococcus aureus infections in a university hospital.Infect Control Hosp Epidemiol. 1992 Oct;13(10):587-93. doi: 10.1086/646433. Infect Control Hosp Epidemiol. 1992. PMID: 1469267 Review.
Cited by
-
Microbiological profile of bloodstream infections and antimicrobial resistance patterns at a tertiary referral hospital in Amazon, Brazil.Rev Soc Bras Med Trop. 2023 Sep 22;56:e03822023. doi: 10.1590/0037-8682-0382-2023. eCollection 2023. Rev Soc Bras Med Trop. 2023. PMID: 37792844 Free PMC article.
-
Risk Factors and Outcomes of Bloodstream Infections Among People With Human Immunodeficiency Virus: A Longitudinal Cohort Study From 2000 to 2017.Open Forum Infect Dis. 2022 Aug 3;9(8):ofac318. doi: 10.1093/ofid/ofac318. eCollection 2022 Aug. Open Forum Infect Dis. 2022. PMID: 35937645 Free PMC article.
References
-
- Laupland K.B., Lyytikainen O., Sogaard M. The changing epidemiology of Staphylococcus aureus bloodstream infection: a multinational population-based surveillance study. Clin Microbiol Infect. 2013;19(5):465–471. - PubMed
-
- Lam J.C., Gregson D.B., Robinson S., Somayaji R., Conly J.M., Parkins M.D. Epidemiology and outcome determinants of staphylococcus aureus bacteremia revisited: a population-based study. Infection. 2019;47(6):961–971. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
