

Neuropathology of COVID-19 (neuro-COVID): clinicopathological update
- PMID: 33554218
- PMCID: PMC7861505
- DOI: 10.17879/freeneuropathology-2021-2993
Neuropathology of COVID-19 (neuro-COVID): clinicopathological update
Abstract
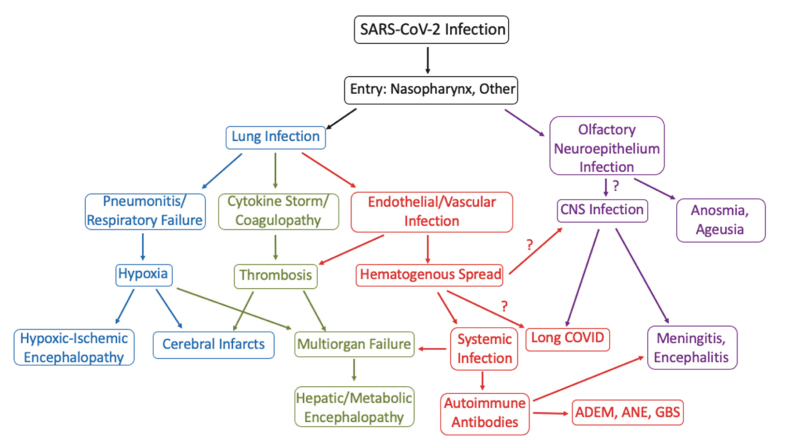
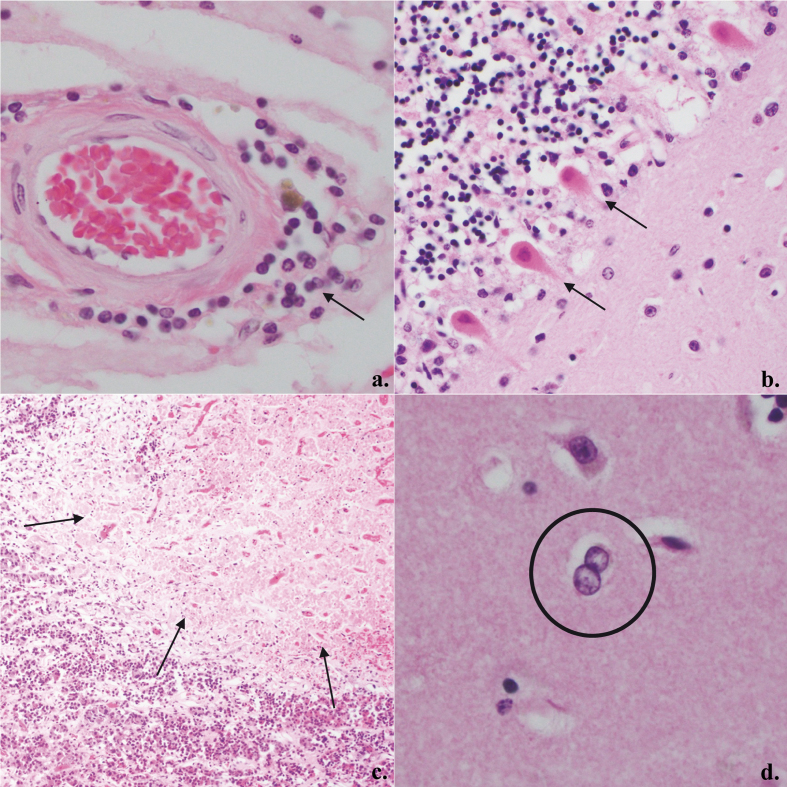
Coronavirus disease 2019 (COVID-19) is emerging as the greatest public health crisis in the early 21stcentury. Its causative agent, Severe Acute Respiratory Syndrome coronavirus 2 (SARS-CoV-2), is an enveloped single stranded positive-sense ribonucleic acid virus that enters cells via the angiotensin converting enzyme 2 receptor or several other receptors. While COVID-19 primarily affects the respiratory system, other organs including the brain can be involved. In Western clinical studies, relatively mild neurological dysfunction such as anosmia and dysgeusia is frequent (~70-84%) while severe neurologic disorders such as stroke (~1-6%) and meningoencephalitis are less common. It is unclear how much SARS-CoV-2 infection contributes to the incidence of stroke given co-morbidities in the affected patient population. Rarely, clinically-defined cases of acute disseminated encephalomyelitis, Guillain-Barré syndrome and acute necrotizing encephalopathy have been reported in COVID-19 patients. Common neuropathological findings in the 184 patients reviewed include microglial activation (42.9%) with microglial nodules in a subset (33.3%), lymphoid inflammation (37.5%), acute hypoxic-ischemic changes (29.9%), astrogliosis (27.7%), acute/subacute brain infarcts (21.2%), spontaneous hemorrhage (15.8%), and microthrombi (15.2%). In our institutional cases, we also note occasional anterior pituitary infarcts. COVID-19 coagulopathy, sepsis, and acute respiratory distress likely contribute to a number of these findings. When present, central nervous system lymphoid inflammation is often minimal to mild, is detected best by immunohistochemistry and, in one study, indistinguishable from control sepsis cases. Some cases evince microglial nodules or neuronophagy, strongly supporting viral meningoencephalitis, with a proclivity for involvement of the medulla oblongata. The virus is detectable by reverse transcriptase polymerase chain reaction, immunohistochemistry, or electron microscopy in human cerebrum, cerebellum, cranial nerves, olfactory bulb, as well as in the olfactory epithelium; neurons and endothelium can also be infected. Review of the extant cases has limitations including selection bias and limited clinical information in some cases. Much remains to be learned about the effects of direct viral infection of brain cells and whether SARS-CoV-2 persists long-term contributing to chronic symptomatology.
Keywords: CNS; COVID-19; SARS-CoV-2; brain; pituitary.
Figures

References
-
- Naming the coronavirus disease (COVID-19) and the virus that causes it. World Health Organization. Accessed October 21, 2020. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technica...
-
- Weekly epidemiological update - 29 December 2020. World Health Organization. Accessed December 30, 2020. https://www.who.int/publications/m/item/weekly-epidemiological-update---...
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous