

COVID-19 in hospitalized liver transplant recipients: An early systematic review and meta-analysis
- PMID: 33555058
- PMCID: PMC7995098
- DOI: 10.1111/ctr.14246
COVID-19 in hospitalized liver transplant recipients: An early systematic review and meta-analysis
Abstract
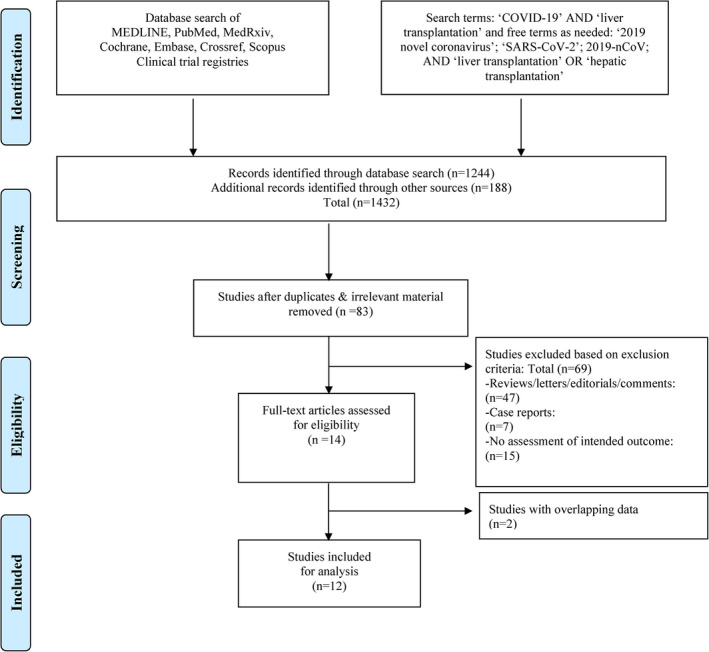
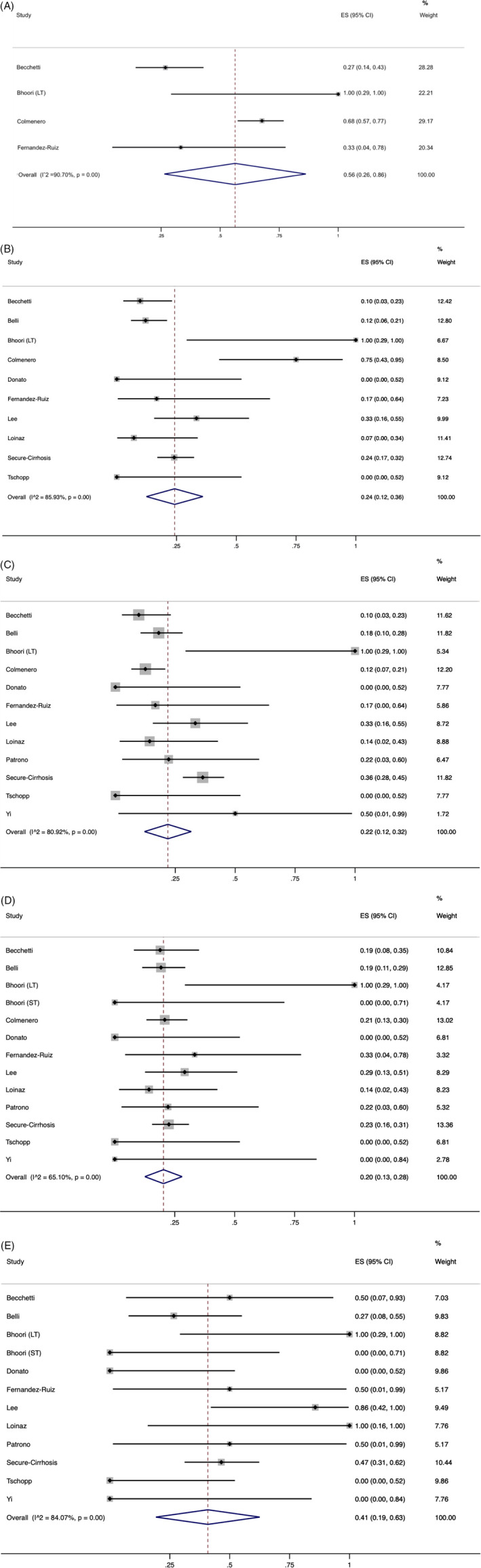
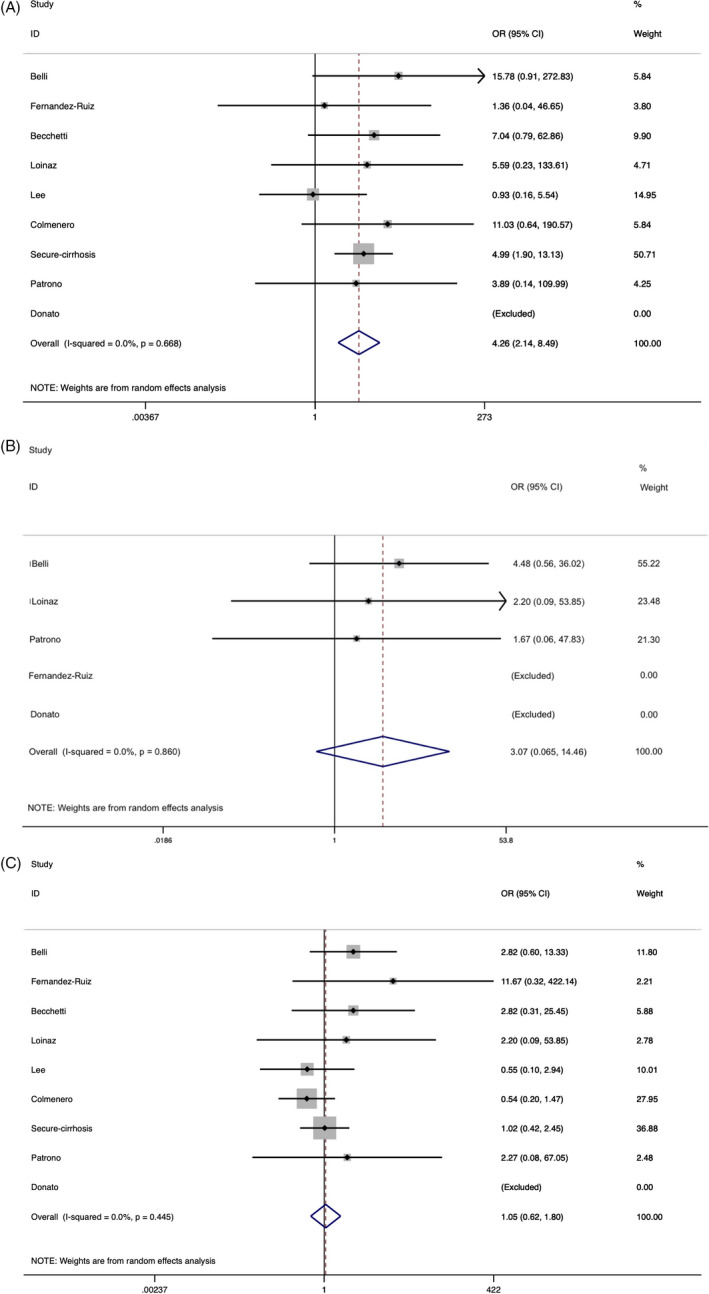
Adverse clinical outcomes related to SARS-CoV-2 infection among liver transplant (LTx) recipients remain undefined. We performed a meta-analysis to determine the pooled prevalence of outcomes among hospitalized LTx recipients with COVID-19. A database search of literature published between December 1, 2019, and November 20, 2020, was performed per PRISMA guidelines. Twelve studies comprising 517 hospitalized LTx recipients with COVID-19 were analyzed. Common presenting symptoms were fever (71%), cough (62%), dyspnea (48%), and diarrhea (28%). Approximately 77% (95% CI, 61%-93%) of LTx recipients had a history of liver cirrhosis. The most prevalent comorbidities were hypertension (55%), diabetes (45%), and cardiac disease (21%). In-hospital mortality was 20% (95% CI, 13%-28%) and rose to 41% (95% CI, 19%-63%) (P < 0.00) with ICU admission. Additional subgroup analysis demonstrated a higher mortality risk in the elderly (>60-65 years) (OR 4.26; 95% CI, 2.14-8.49). There was no correlation in respect to sex or time since transplant. In summary, LTx recipients with COVID-19 had a high prevalence of dyspnea and gastrointestinal symptoms. In-hospital mortality was comparable to non-transplant populations with similar comorbidities but appeared to be less than what is reported elsewhere for cirrhotic patients (26%-40%). Importantly, the observed high case fatality in the elderly could be due to age-associated comorbidities.
Keywords: COVID-19; SARS-CoV-2; liver transplantation.
© 2021 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd.
Conflict of interest statement
None of the authors reported any conflicts of interest, including no specific financial interests or relationships and affiliations relevant to the subject matter or materials discussed in the manuscript.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
