

Association of Preexisting Disability With Severe Maternal Morbidity or Mortality in Ontario, Canada
- PMID: 33555330
- PMCID: PMC7871190
- DOI: 10.1001/jamanetworkopen.2020.34993
Association of Preexisting Disability With Severe Maternal Morbidity or Mortality in Ontario, Canada
Abstract
Importance: Severe maternal morbidity and mortality are important indicators of maternal health. Pregnancy rates are increasing in women with disabilities, but their risk of severe maternal morbidity and mortality is unknown, despite their significant social and health disparities.
Objective: To determine the risk of severe maternal morbidity or mortality among women with a physical, sensory, or intellectual/developmental disability compared with women without disabilities.
Design, setting, and participants: This population-based cohort study used linked health administrative data in Ontario, Canada, from 2003 to 2018. The cohort included all singleton births to women with preexisting physical, sensory, and intellectual/developmental disabilities as well as with 2 disabilities or more compared with women without a disability. Data analysis was conducted from September 2019 to September 2020.
Exposures: Disabilities were identified with published algorithms applied to diagnoses in 2 physician visits or more or at least 1 emergency department visit or hospitalization.
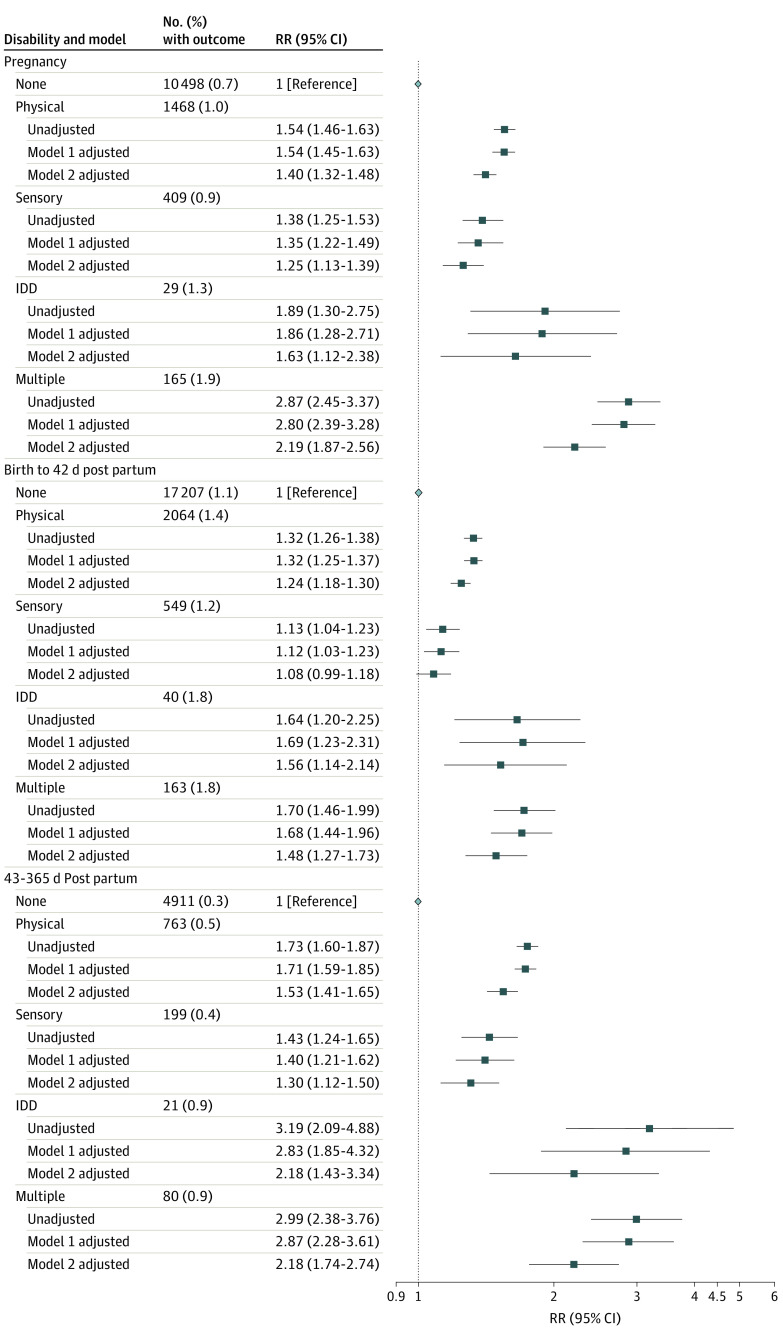
Main outcomes and measures: Severe maternal morbidity (a validated composite of 40 diagnostic and procedural indicators) or all-cause maternal mortality, arising between conception and 42 days post partum. Relative risks were adjusted for maternal age, parity, income quintile, rurality, chronic medical conditions, mental illness, and substance use disorders.
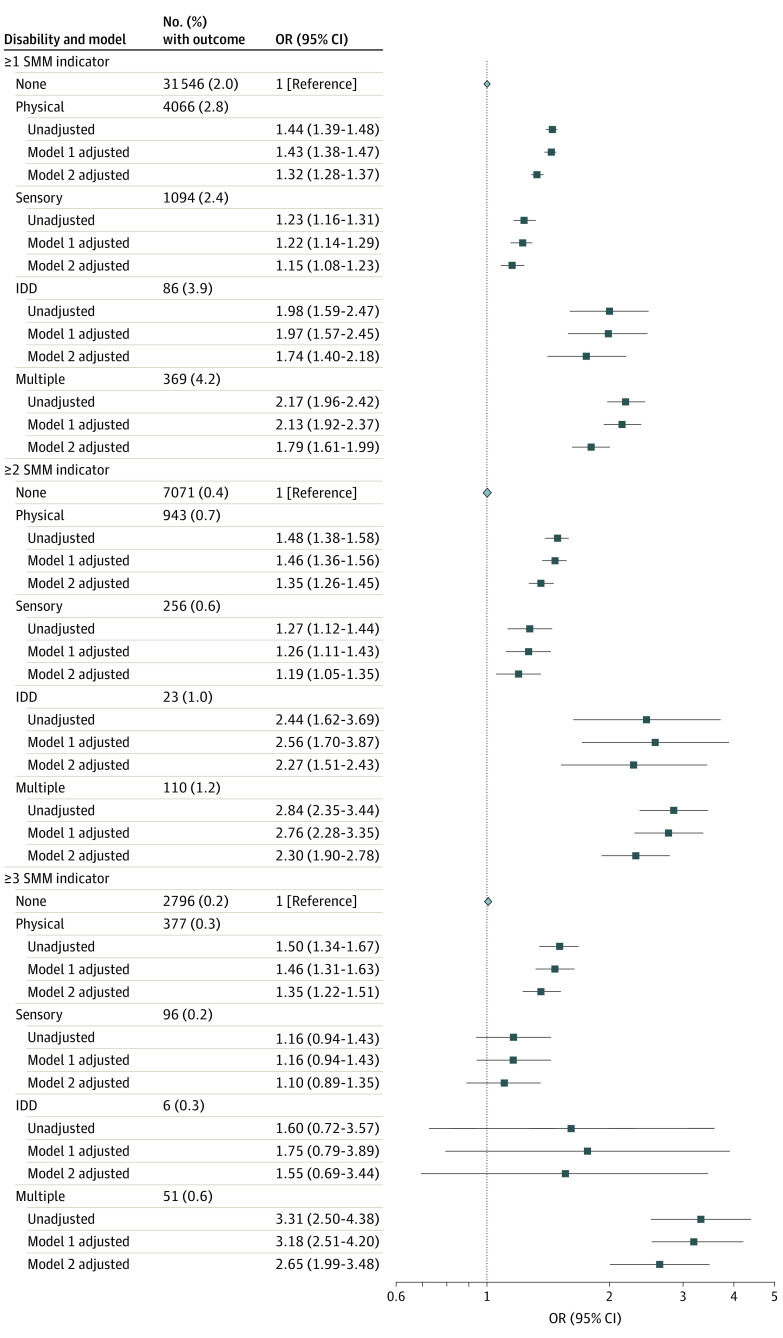
Results: The cohort comprised women with physical disabilities (144 972 women; mean [SD] age, 29.8 [5.6] years), sensory disabilities (45 259 women; mean [SD] age, 29.1 [6.0] years), intellectual/developmental disabilities (2227 women; mean [SD] age, 26.1 [6.4] years), and 2 or more disabilities (8883 women; mean [SD] age, 29.1 [6.1] years), and those without disabilities (1 601 363 women; mean [SD] age, 29.6 [5.4] years). The rate of severe maternal morbidity or death was 1.7% (27 242 women) in women without a disability. Compared with these women, the risk of severe maternal morbidity or death was higher in women with a physical disability (adjusted relative risk [aRR], 1.29; 95% CI, 1.25-1.34), a sensory disability (aRR, 1.14; 95% CI, 1.06-1.21), an intellectual/developmental disability (aRR, 1.57; 95% CI, 1.23-2.01), and 2 or more disabilities (aRR, 1.74; 95% CI, 1.55-1.95). Similar aRRs were observed for severe maternal morbidity or death arising in pregnancy, from birth to 42 days post partum, and from 43 to 365 days post partum. Women with disabilities were more likely than those without disabilities to experience multiple severe maternal morbidity indicators. The most prevalent indicators in all groups were intensive care unit admission, severe postpartum hemorrhage, puerperal sepsis, and severe preeclampsia.
Conclusions and relevance: In this study, women with a preexisting disability were more likely to experience severe maternal morbidity or mortality. Preconception and perinatal care provisions should be considered among women with a disability to mitigate the risk of these rare but serious outcomes.
Conflict of interest statement
Figures
Comment in
-
Understanding Reproductive Outcomes Among Women With Disabilities.JAMA Netw Open. 2021 Feb 1;4(2):e2035121. doi: 10.1001/jamanetworkopen.2020.35121. JAMA Netw Open. 2021. PMID: 33555327 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
