

Prognostic value of NT-proBNP for myocardial recovery in peripartum cardiomyopathy (PPCM)
- PMID: 33555408
- PMCID: PMC8318939
- DOI: 10.1007/s00392-021-01808-z
Prognostic value of NT-proBNP for myocardial recovery in peripartum cardiomyopathy (PPCM)
Abstract
Introduction: Peripartum cardiomyopathy (PPCM) is an important cause of pregnancy-associated heart failure worldwide. Although a significant number of women recover their left ventricular (LV) function within 12 months, some remain with persistently reduced systolic function.
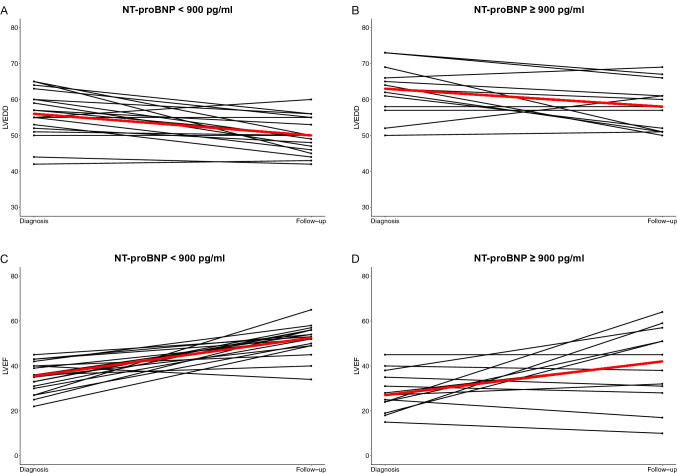
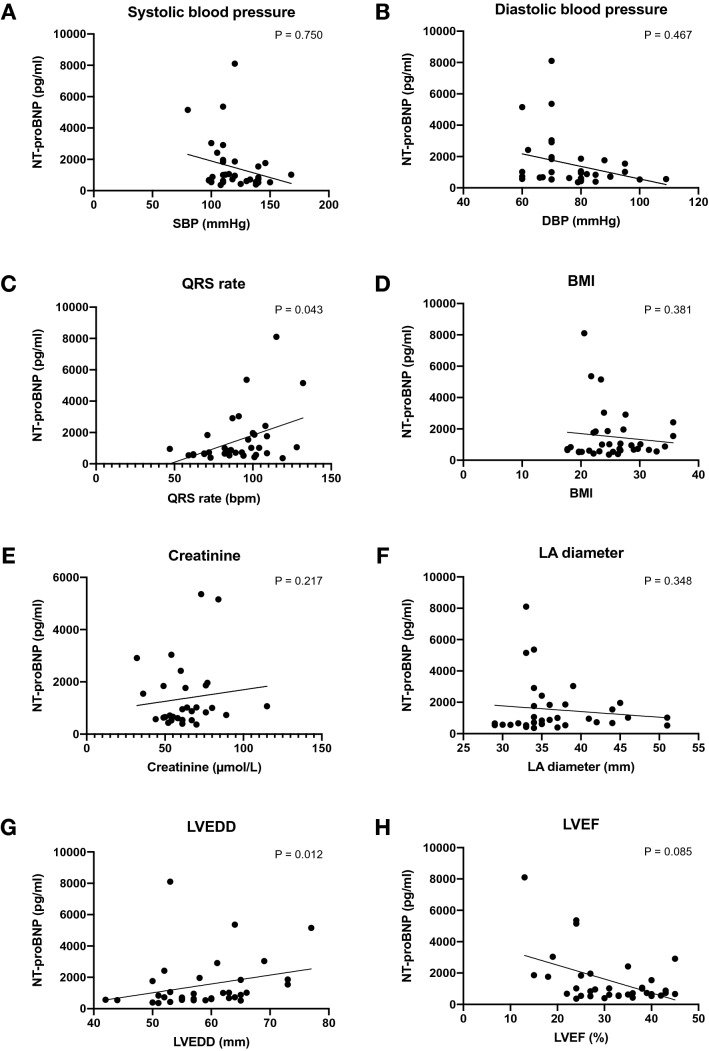
Methods: Knowledge gaps exist on predictors of myocardial recovery in PPCM. N-terminal pro-brain natriuretic peptide (NT-proBNP) is the only clinically established biomarker with diagnostic value in PPCM. We aimed to establish whether NT-proBNP could serve as a predictor of LV recovery in PPCM, as measured by LV end-diastolic volume (LVEDD) and LV ejection fraction (LVEF).
Results: This study of 35 women with PPCM (mean age 30.0 ± 5.9 years) had a median NT-proBNP of 834.7 pg/ml (IQR 571.2-1840.5) at baseline. Within the first year of follow-up, 51.4% of the cohort recovered their LV dimensions (LVEDD < 55 mm) and systolic function (LVEF > 50%). Women without LV recovery presented with higher NT-proBNP at baseline. Multivariable regression analyses demonstrated that NT-proBNP of ≥ 900 pg/ml at the time of diagnosis was predictive of failure to recover LVEDD (OR 0.22, 95% CI 0.05-0.95, P = 0.043) or LVEF (OR 0.20 [95% CI 0.04-0.89], p = 0.035) at follow-up.
Conclusions: We have demonstrated that NT-proBNP has a prognostic value in predicting LV recovery of patients with PPCM. Patients with NT-proBNP of ≥ 900 pg/ml were less likely to show any improvement in LVEF or LVEDD. Our findings have implications for clinical practice as patients with higher NT-proBNP might require more aggressive therapy and more intensive follow-up. Point-of-care NT-proBNP for diagnosis and risk stratification warrants further investigation.
Keywords: Heart failure; Left ventricular recovery; NT-proBNP; Peripartum cardiomyopathy; Risk stratification.
© 2021. The Author(s).
Conflict of interest statement
The authors have no conflicting interests to disclose.
Figures
References
-
- Sliwa K, Hilfiker-Kleiner D, Petrie MC, Mebazaa A, Pieske B, Buchmann E, et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of peripartum cardiomyopathy: a position statement from the Heart Failure Association of the European Society of Cardiology Working Group on peripartum cardiomyopathy. Eur J Heart Fail. 2010;12(8):767–778. doi: 10.1093/eurjhf/hfq120. - DOI - PubMed
-
- Bauersachs J, Konig T, van der Meer P, Petrie MC, Hilfiker-Kleiner D, Mbakwem A, et al. Pathophysiology, diagnosis and management of peripartum cardiomyopathy: a position statement from the Heart Failure Association of the European Society of Cardiology Study Group on peripartum cardiomyopathy. Eur J Heart Fail. 2019;21(7):827–843. doi: 10.1002/ejhf.1493. - DOI - PubMed
-
- Goland S, Bitar F, Modi K, Safirstein J, Ro A, Mirocha J, et al. Evaluation of the clinical relevance of baseline left ventricular ejection fraction as a predictor of recovery or persistence of severe dysfunction in women in the United States with peripartum cardiomyopathy. J Card Fail. 2011;17(5):426–430. doi: 10.1016/j.cardfail.2011.01.007. - DOI - PubMed
-
- McNamara DM, Elkayam U, Alharethi R, Damp J, Hsich E, Ewald G, et al. Clinical outcomes for peripartum cardiomyopathy in North America: results of the IPAC Study (Investigations of pregnancy-associated cardiomyopathy) J Am Coll Cardiol. 2015;66(8):905–914. doi: 10.1016/j.jacc.2015.06.1309. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
