

The role of ultrasound imaging in vascular compression syndromes
- PMID: 33555480
- PMCID: PMC7870731
- DOI: 10.1186/s13089-020-00202-6
The role of ultrasound imaging in vascular compression syndromes
Abstract
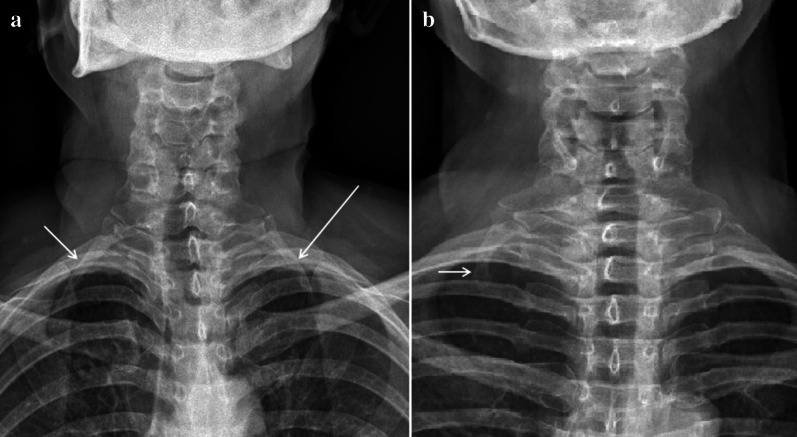
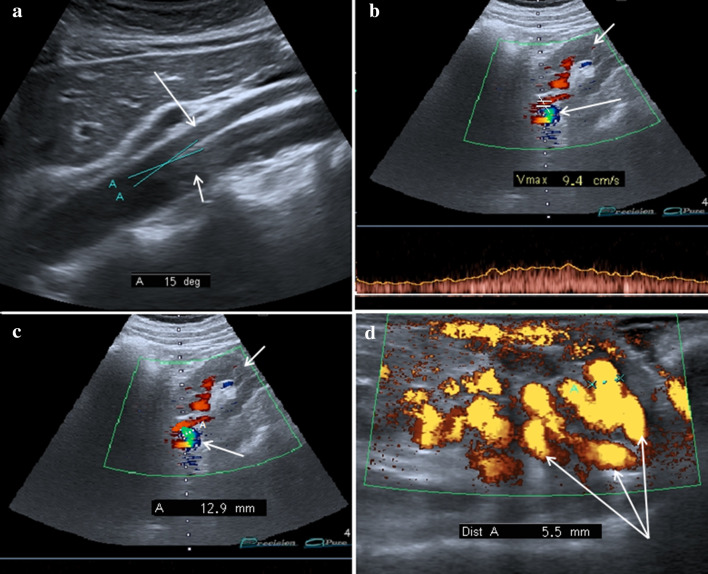
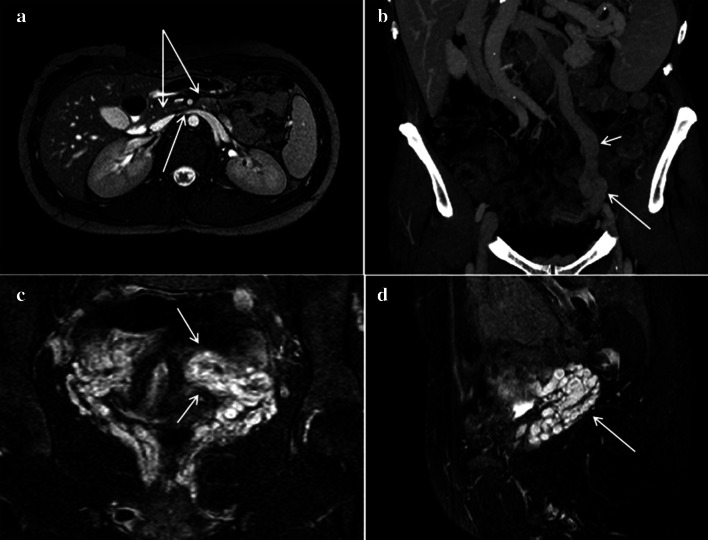
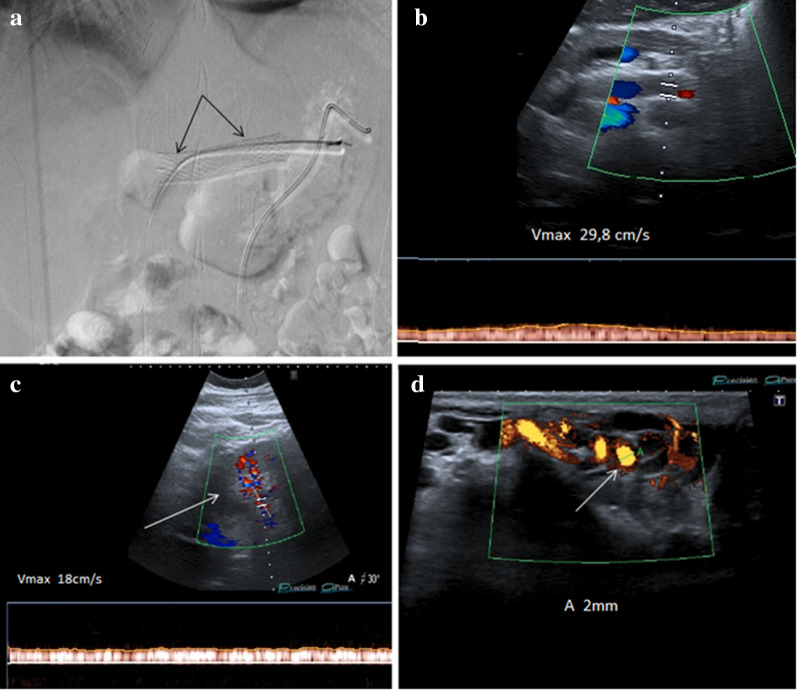
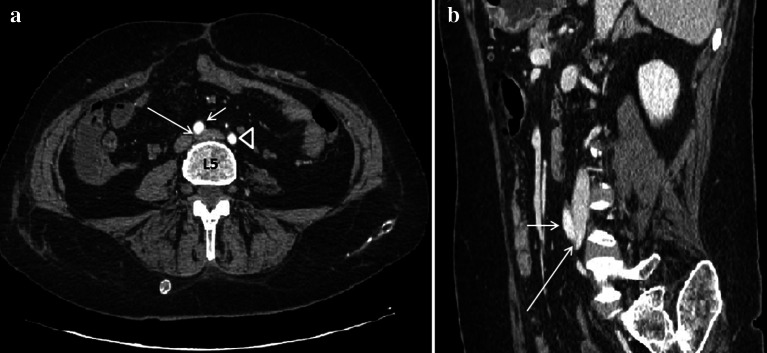
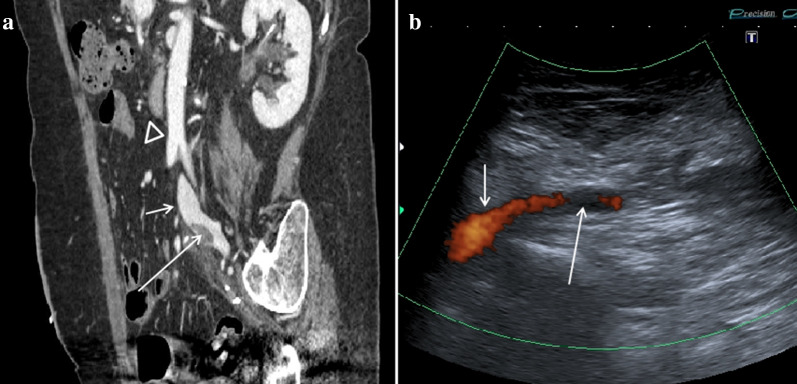
Vascular compression syndromes are rare alterations that have in common the compression of an arterial and/or venous vessel by contiguous structures and can be congenital or acquired. The best known are the Thoracic Outlet Syndrome, Nutcracker Syndrome, May-Thurner Syndrome, and Dunbar Syndrome. The incidence of these pathologies is certainly underestimated due to the non-specific clinical signs and their frequent asymptomaticity. Being a first-level method, Ultrasound plays a very important role in identifying these alterations, almost always allowing a complete diagnostic classification. If in expert hands, this method can significantly contribute to the reduction of false negatives, especially in the asymptomatic population, where the finding of the aforementioned pathologies often happens randomly following routine checks. In this review, we briefly discuss the best known vascular changes, the corresponding ultrasound anatomy, and typical ultrasound patterns.
Keywords: Abdominal ultrasound; Color Doppler ultrasound; Dunbar syndrome; Duplex Doppler ultrasound; May–Thurner syndrome; Nutcracker syndrome.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures












References
-
- Pesser N, Teijink JAW, Vervaart K et al. (2020) Value of Ultrasound in the Diagnosis of Neurogenic Thoracic Outlet Syndrome. Eur J Vasc Endovasc Surg. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources