

Efficacy of early anti-inflammatory treatment with high doses of intravenous anakinra with or without glucocorticoids in patients with severe COVID-19 pneumonia
- PMID: 33556464
- PMCID: PMC7865089
- DOI: 10.1016/j.jaci.2021.01.024
Efficacy of early anti-inflammatory treatment with high doses of intravenous anakinra with or without glucocorticoids in patients with severe COVID-19 pneumonia
Abstract
Background: IL-1 plays a pivotal role in the inflammatory response during cytokine storm syndromes.
Objective: Our aim was to analyze the efficacy and safety of early anti-inflammatory treatment (AIT) with intravenous anakinra with or without glucocorticoids in coronavirus disease 2019 (COVID-19) pneumonia.
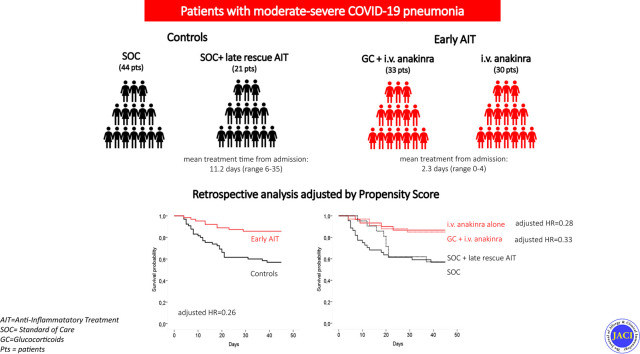
Methods: We performed a retrospective single-center cohort study of patients admitted for COVID-19 pneumonia from February 26 to April 29, 2020, to assess the efficacy of early AIT with intravenous anakinra (100 mg every 8 hours for 3 days, with tapering) alone or in combination with a glucocorticoid (intravenous methylprednisolone, 1-2 mg/kg daily, with tapering). The standard of care (SOC) treatment was hydroxychloroquine and/or azithromycin with or without antivirals and anticoagulants. Late rescue AIT with anakinra or tocilizumab was also evaluated. Treatment effect on overall survival was assessed by a propensity score-adjusted Cox model.
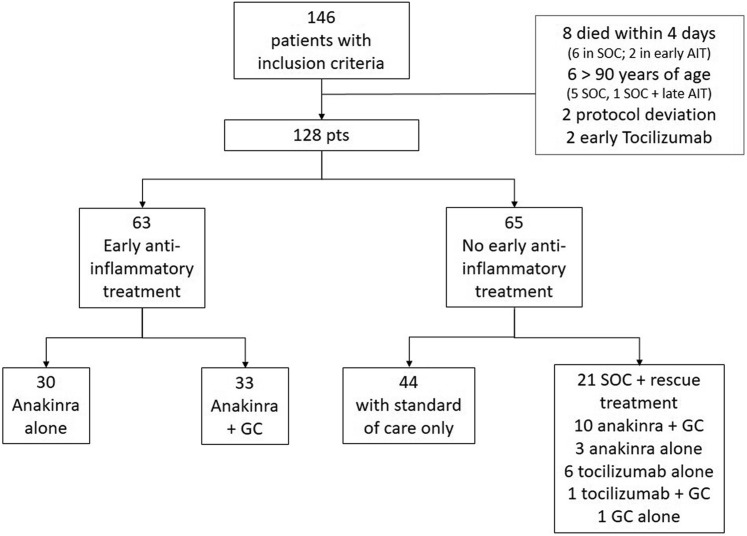
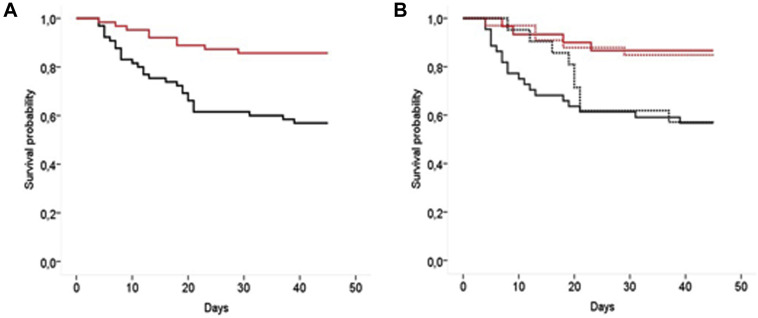
Results: A total of 128 patients were analyzed; 63 patients received early AIT (30 received anakinra alone and 33 received anakinra plus a glucocorticoid) at admission, and 65 patients did not receive early AIT and were used as controls; of the latter 65 patients, 44 received the SOC treatment alone and 21 received the SOC treatment plus late rescue AIT. After adjustment for all the unbalanced baseline covariates, early AIT reduced the hazard of mortality by 74% (adjusted hazard ratio [HR] = 0.26; P < .001). The effect was similar in patients receiving anakinra alone (adjusted HR = 0.28; P = .04) and anakinra plus a glucocorticoid (adjusted HR = 0.33; P = .07). Late rescue treatment did not show a significant advantage over SOC treatment alone (adjusted HR = 0.82; P = .70).
Conclusions: This study suggests, on a larger series of patients with COVID-19 pneumonia, the potential efficacy and safety of the early use of high doses of intravenous anakinra with or without glucocorticoids.
Keywords: COVID-19 pneumonia; IL-1; anakinra; early treatment; glucocorticoid.
Copyright © 2021 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Ravelli A., Davì S., Minoia F., Martini A., Cron R.Q. Macrophage activation syndrome. Hematol Oncol Clin North Am. 2015;29:927–941. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
