

Predicted Versus Non-Predicted Opioid Administration Using Preoperative Pain Sensitivity in Patients Undergoing Gynecological Surgery: A Randomized-Controlled Trial
- PMID: 33557259
- PMCID: PMC7914520
- DOI: 10.3390/jcm10040585
Predicted Versus Non-Predicted Opioid Administration Using Preoperative Pain Sensitivity in Patients Undergoing Gynecological Surgery: A Randomized-Controlled Trial
Abstract
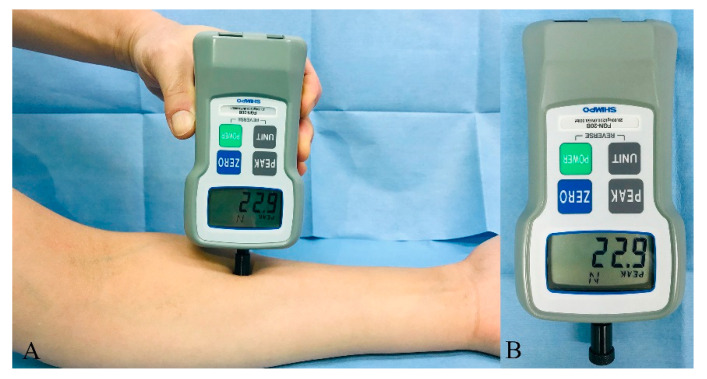
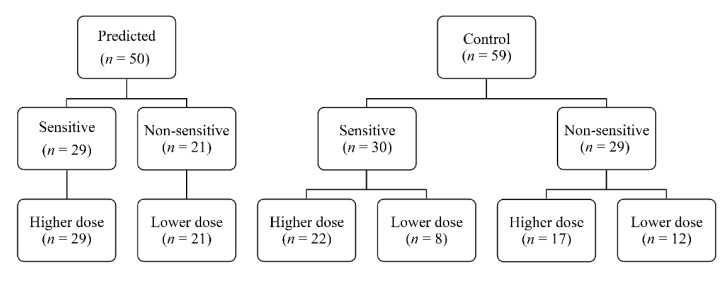
Individualized administration of opioids based on preoperative pain sensitivity may improve postoperative pain profiles. This study aimed to examine whether a predicted administration of opioids could reduce opioid-related adverse effects after gynecological surgery. Patients were randomized to the predicted group or control group. Participants received a preoperative sensory test to measure pressure pain thresholds. Patients were treated with a higher or lower (15 or 10 μg/mL) dose of fentanyl via intravenous patient-controlled analgesia. The opioid dose was determined according to pain sensitivity in the predicted group, while it was determined regardless of pain sensitivity in the control group. The primary outcome was the incidence of nausea over the first 48 h postoperative period. Secondary outcomes included postoperative pain scores and opioid requirements. There was no difference in the incidence of nausea (40.0% vs. 52.5% in predicted and control groups, respectively; p = 0.191) and postoperative pain scores (3.3 vs. 3.5 in predicted and control groups, respectively; p = 0.691). However, opioid consumptions were lower in the predicted group compared to the control group (median 406.0 vs. 526.5 μg; p = 0.042). This study showed that offering a predicted dose of opioids according to pain sensitivity did not affect the incidence of nausea and pain scores.
Keywords: intravenous patient-controlled analgesia; nausea; opioid; postoperative pain.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Aubrun F., Zahr N., Langeron O., Boccheciampe N., Cozic N., Belin L., Hulot J.S., Khiami F., Riou B. Opioid-related genetic polymorphisms do not influence postoperative opioid requirement: A prospective observational study. Eur. J. Anaesthesiol. 2018;35:496–504. doi: 10.1097/EJA.0000000000000793. - DOI - PubMed
-
- Nelson G., Bakkum-Gamez J., Kalogera E., Glaser G., Altman A., Meyer L.A., Taylor J.S., Iniesta M., Lasala J., Mena G., et al. Guidelines for perioperative care in gynecologic/oncology: Enhanced Recovery After Surgery (ERAS) Society recommendations-2019 update. Int. J. Gynecol. Cancer. 2019 doi: 10.1136/ijgc-2019-000356. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
