

Accelerated Wound Closure of Deep Partial Thickness Burns with Acellular Fish Skin Graft
- PMID: 33557424
- PMCID: PMC7915828
- DOI: 10.3390/ijms22041590
Accelerated Wound Closure of Deep Partial Thickness Burns with Acellular Fish Skin Graft
Abstract
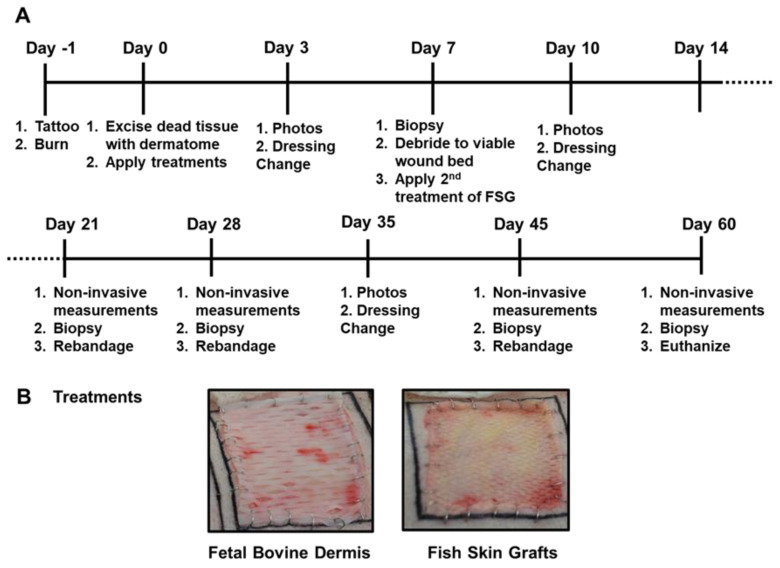
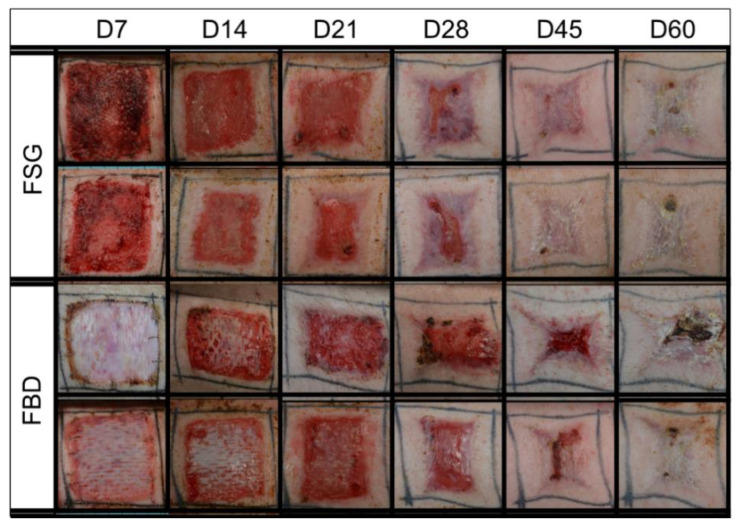
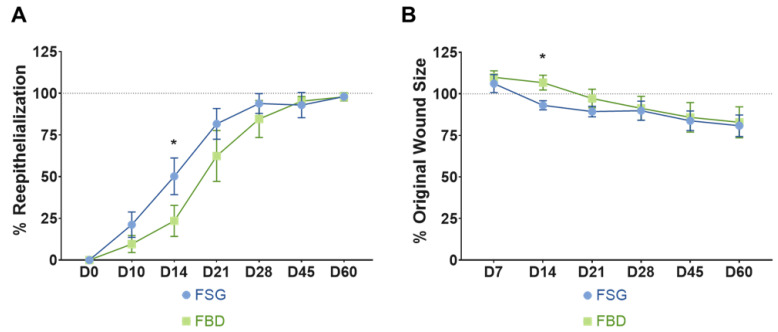
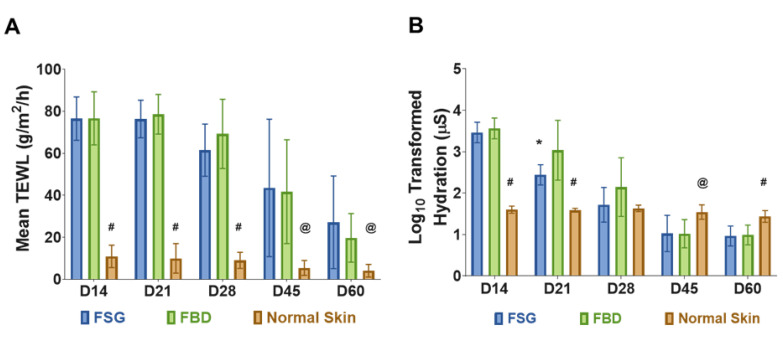
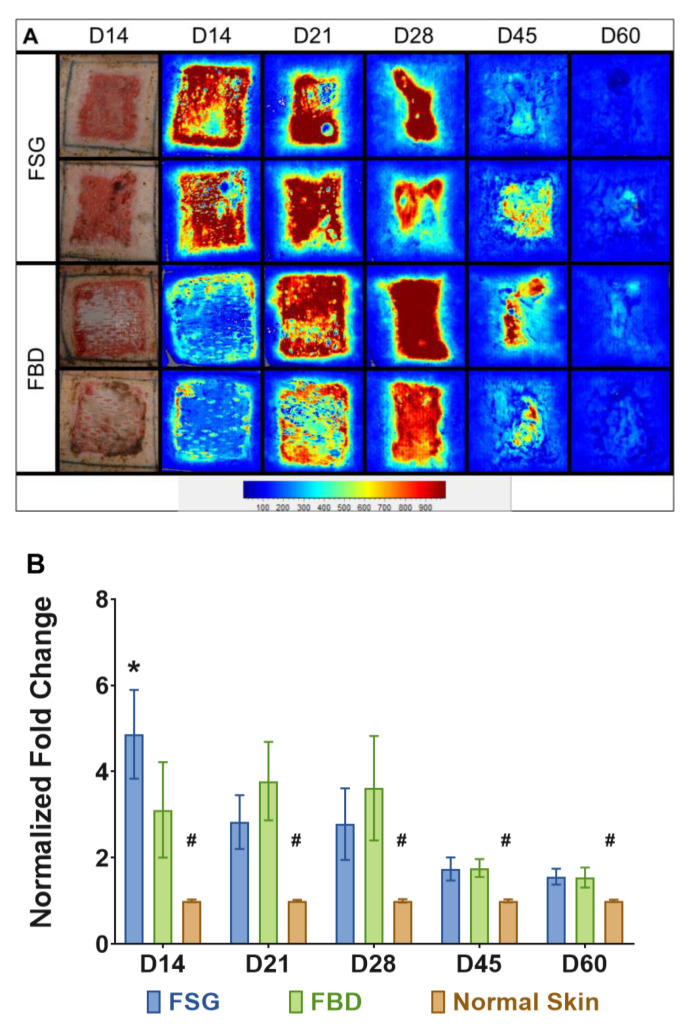
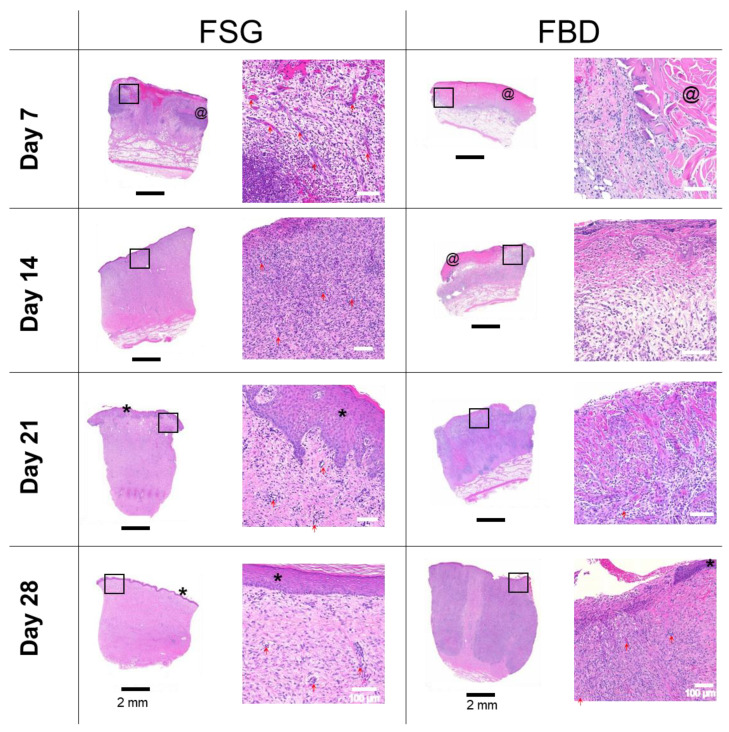
Thermal injuries are caused by exposure to a variety of sources, and split thickness skin grafts are the gold standard treatment for severe burns; however, they may be impossible when there is no donor skin available. Large total body surface area burns leave patients with limited donor site availability and create a need for treatments capable of achieving early and complete coverage that can also retain normal skin function. In this preclinical trial, two cellular and tissue based products (CTPs) are evaluated on twenty-four 5 × 5 deep partial thickness (DPT) burn wounds. Using appropriate pain control methods, DPT burn wounds were created on six anesthetized Yorkshire pigs. Wounds were excised one day post-burn and the bleeding wound beds were subsequently treated with omega-3-rich acellular fish skin graft (FSG) or fetal bovine dermis (FBD). FSG was reapplied after 7 days and wounds healed via secondary intentions. Digital images, non-invasive measurements, and punch biopsies were acquired during rechecks performed on days 7, 14, 21, 28, 45, and 60. Multiple qualitative measurements were also employed, including re-epithelialization, contraction rates, hydration, laser speckle, and trans-epidermal water loss (TEWL). Each treatment produced granulated tissue (GT) that would be receptive to skin grafts, if desired; however, the FSG induced GT 7 days earlier. FSG treatment resulted in faster re-epithelialization and reduced wound size at day 14 compared to FBD (50.2% vs. 23.5% and 93.1% vs. 106.7%, p < 0.005, respectively). No differences in TEWL measurements were observed. The FSG integrated into the wound bed quicker as evidenced by lower hydration values at day 21 (309.7 vs. 2500.4 µS, p < 0.05) and higher blood flow at day 14 (4.9 vs. 3.1 fold change increase over normal skin, p < 0.005). Here we show that FSG integrated faster without increased contraction, resulting in quicker wound closure without skin graft application which suggests FSG improved burn wound healing over FBD.
Keywords: burn; cellular and tissue-based product; contraction; epithelialization; fetal bovine dermis; fish skin graft; swine.
Conflict of interest statement
S.M and H.K. are employees of Kerecis®, Reykjavik, Iceland. For the remaining authors none are declared.
Figures
References
-
- American Burn Association; 2016. [(accessed on 15 October 2020)]. Burn Incidence and Treatment in the United States: 2016 Fact. Sheet. Available online: http://ameriburn.org/who-we-are/media/burn-incidence-fact-sheet/
-
- Tam J., Wang Y., Farinelli W.A., Jiménez-Lozano J., Franco W., Sakamoto F.H., Cheung E.J., Purschke M., Doukas A.G., Anderson R.R. Fractional Skin Harvesting: Autologous Skin Grafting without Donor-site Morbidity. Plast. Reconstr. Surg. Glob. Open. 2013;1:e47. doi: 10.1097/GOX.0b013e3182a85a36. - DOI - PMC - PubMed
-
- Garg K., Kaszubski P.A., Moridzadeh R., Rockman C.B., Adelman M.A., Maldonado T.S., Veith F.J., Mussa F.F. Endovascular-first approach is not associated with worse amputation-free survival in appropriately selected patients with critical limb ischemia. J. Vasc Surg. 2014;59:392–399. doi: 10.1016/j.jvs.2013.09.001. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
