

Minimally Invasive Scoliosis Surgery Is a Feasible Option for Management of Idiopathic Scoliosis and Has Equivalent Outcomes to Open Surgery: A Meta-Analysis
- PMID: 33557618
- PMCID: PMC9121169
- DOI: 10.1177/2192568220988267
Minimally Invasive Scoliosis Surgery Is a Feasible Option for Management of Idiopathic Scoliosis and Has Equivalent Outcomes to Open Surgery: A Meta-Analysis
Abstract
Study design: Meta-analysis.
Objective: To compare outcomes between minimally invasive scoliosis surgery (MISS) and traditional posterior instrumentation and fusion in the correction of adolescent idiopathic scoliosis (AIS).
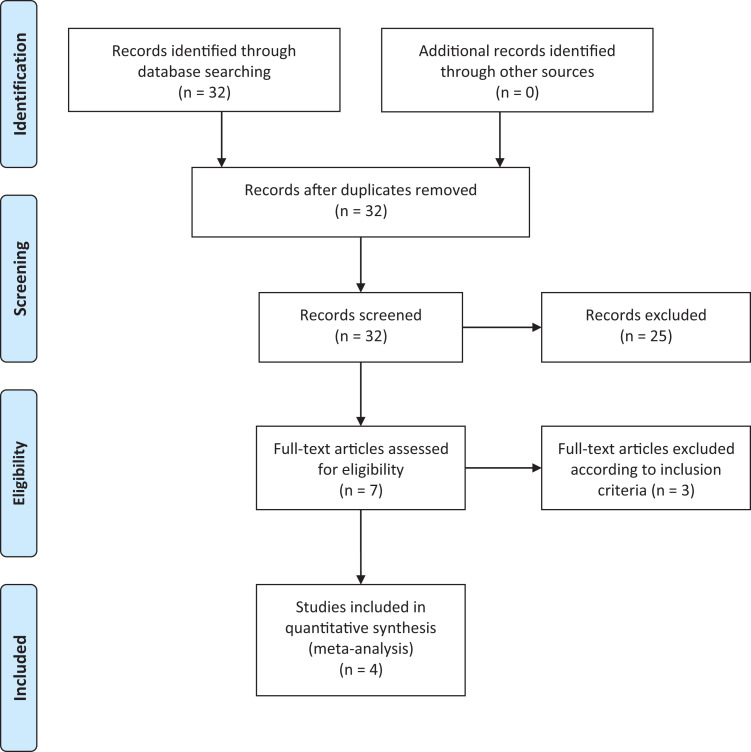
Methods: A literature search was performed using MEDLINE, PubMed, EMBASE, Google scholar and Cochrane databases, including studies reporting outcomes for both MISS and open correction of AIS. Study details, demographics, and outcomes, including curve correction, estimated blood loss (EBL), operative time, postoperative pain, length of stay (LOS), and complications, were collected and analyzed.
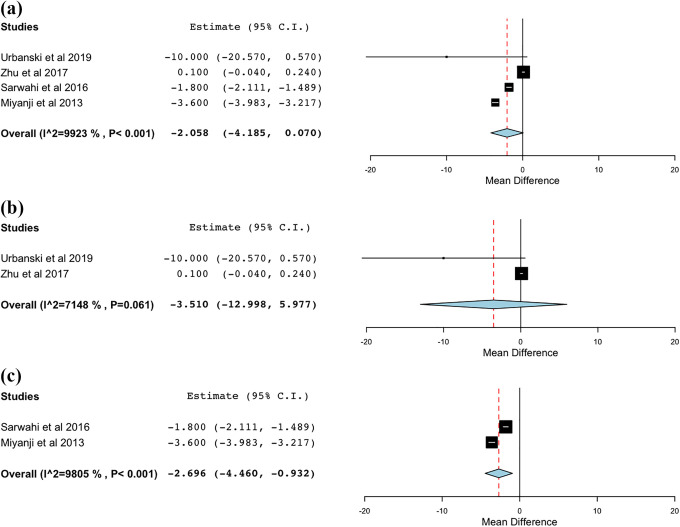
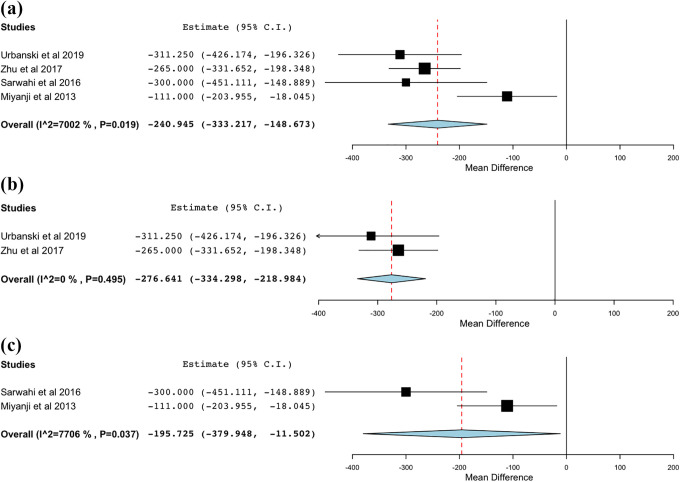
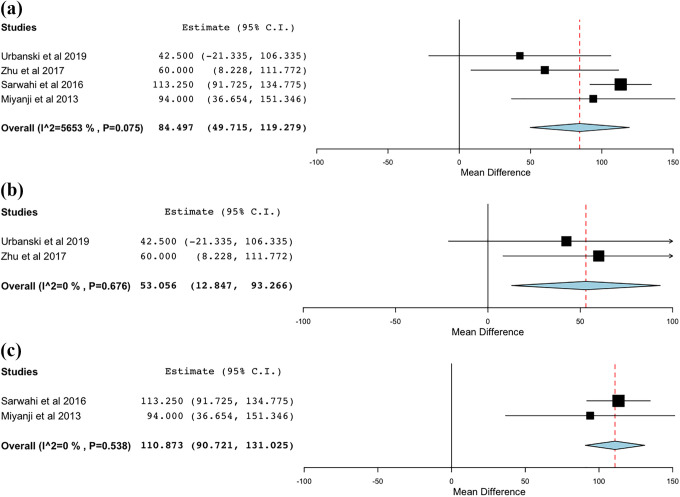
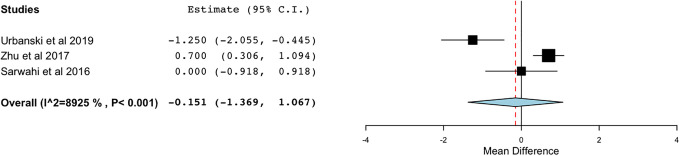
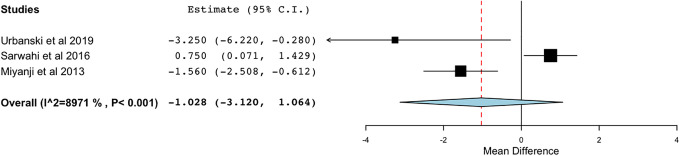
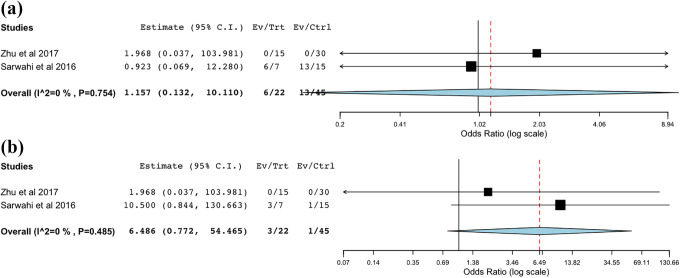
Results: A total of 4 studies met the selection criteria and were included in the analysis, totaling 107 patients (42 MIS and 65 open) with a mean age of 16 years. Overall there was no difference in curve correction between MISS (73.2%) and open (76.7%) cohorts. EBL was significantly lower in the MISS (271 ml) compared to the open (527 ml) group, but operative time was significantly longer (380 min for MISS versus 302 min for open). There were no significant differences between the approaches in pain, LOS, complications, or reoperations.
Conclusion: MISS was associated with less blood loss but longer operative times compared to traditional open fusion for AIS. There was no difference in curve correction, postoperative pain, LOS, or complications/reoperations. While MISS has emerged as a feasible option for the surgical management of AIS, further research is warranted to compare these 2 approaches.
Keywords: adolescent idiopathic scoliosis; idiopathic scoliosis; minimally invasive scoliosis surgery; minimally invasive surgery; open surgery; posterior fusion; spinal fusion.
Conflict of interest statement
Figures
References
-
- Yaman O, Dalbayrak S. Idiopathic scoliosis. Turk Neurosurg. 2014;24(5):646–657. doi:10.5137/1019-5149.JTN.8838-13.0 - PubMed
-
- Shakil H, Iqbal ZA, Al-Ghadir AH. Scoliosis: review of types of curves, etiological theories and conservative treatment. J Back Musculoskelet Rehabil. 2014;27(2):111–115. doi:10.3233/bmr-130438 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
