

Stillbirth outcome capture and classification in population-based surveys: EN-INDEPTH study
- PMID: 33557841
- PMCID: PMC7869203
- DOI: 10.1186/s12963-020-00239-8
Stillbirth outcome capture and classification in population-based surveys: EN-INDEPTH study
Abstract
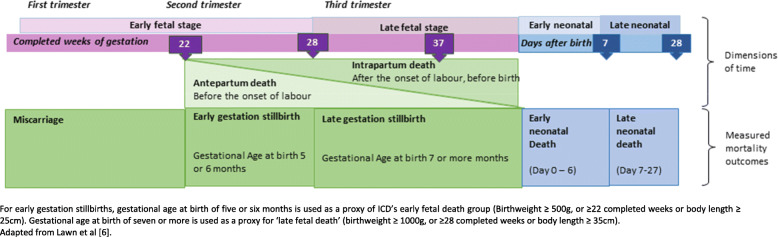
Background: Household surveys remain important sources of stillbirth data, but omission and misclassification are common. Classifying adverse pregnancy outcomes as stillbirths requires accurate reporting of vital status at birth and gestational age or birthweight for every pregnancy. Further categorisation, e.g. by sex, or timing (intrapartum/antepartum) improves data to understand and prevent stillbirth.
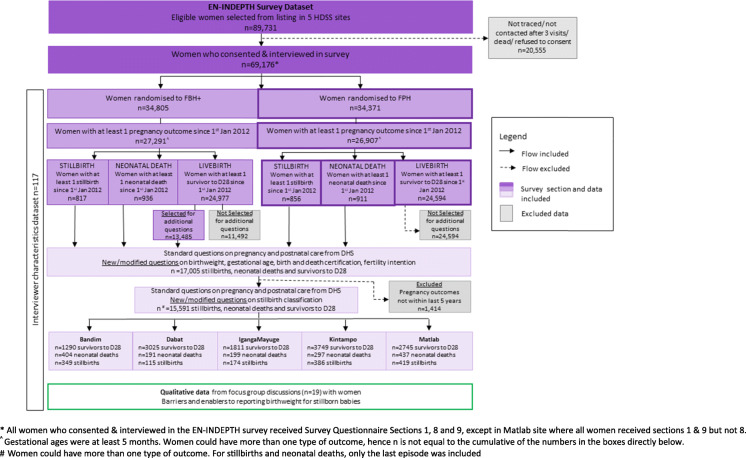
Methods: We undertook a cross-sectional population-based survey of women of reproductive age in five health and demographic surveillance system sites in Bangladesh, Ethiopia, Ghana, Guinea-Bissau and Uganda (2017-2018). All women answered a full birth history with pregnancy loss questions (FBH+) or a full pregnancy history (FPH). A sub-sample across both groups were asked additional stillbirth questions. Questions were evaluated using descriptive measures. Using an interpretative paradigm and phenomenology methodology, focus group discussions with women exploring barriers to reporting birthweight for stillbirths were conducted. Thematic analysis was guided by an a priori codebook.
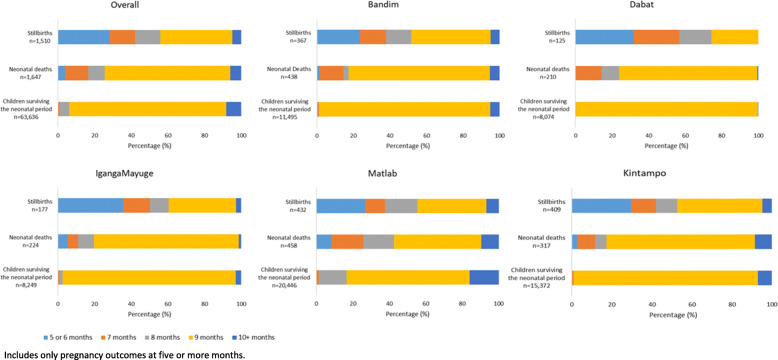
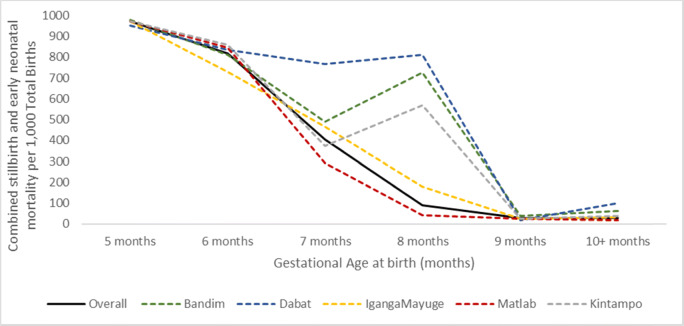
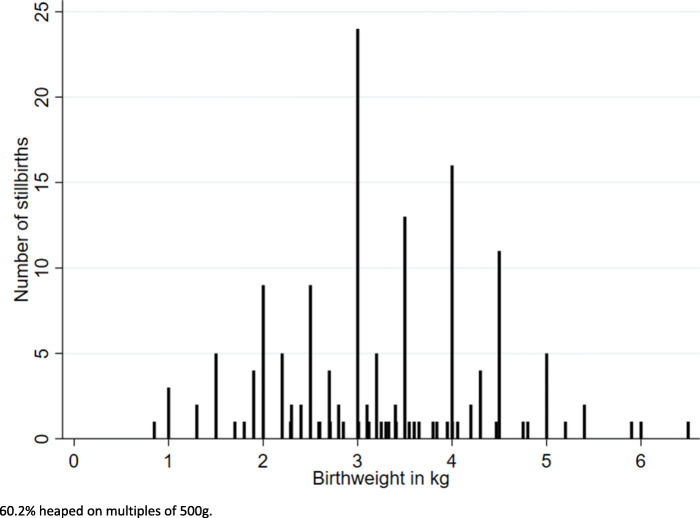
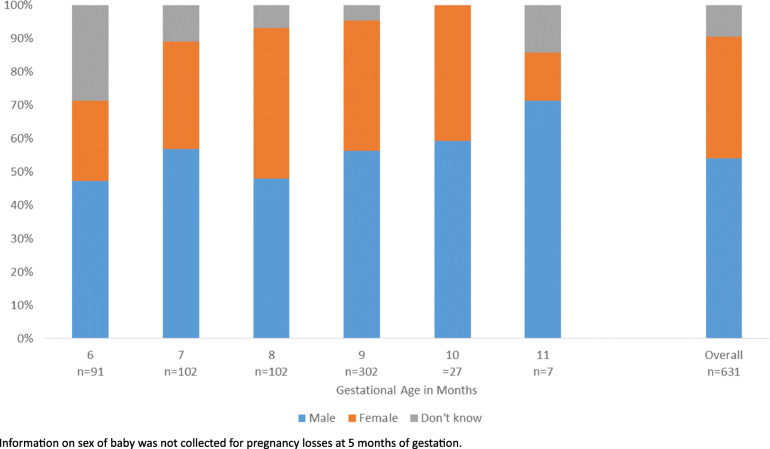
Results: Overall 69,176 women reported 98,483 livebirths (FBH+) and 102,873 pregnancies (FPH). Additional questions were asked for 1453 stillbirths, 1528 neonatal deaths and 12,620 surviving children born in the 5 years prior to the survey. Completeness was high (> 99%) for existing FBH+/FPH questions on signs of life at birth and gestational age (months). Discordant responses in signs of life at birth between different questions were common; nearly one-quarter classified as stillbirths on FBH+/FPH were reported born alive on additional questions. Availability of information on gestational age (weeks) (58.1%) and birthweight (13.2%) was low amongst stillbirths, and heaping was common. Most women (93.9%) were able to report the sex of their stillborn baby. Response completeness for stillbirth timing (18.3-95.1%) and estimated proportion intrapartum (15.6-90.0%) varied by question and site. Congenital malformations were reported in 3.1% stillbirths. Perceived value in weighing a stillborn baby varied and barriers to weighing at birth a nd knowing birthweight were common.
Conclusions: Improving stillbirth data in surveys will require investment in improving the measurement of vital status, gestational age and birthweight by healthcare providers, communication of these with women, and overcoming reporting barriers. Given the large burden and effect on families, improved data must be made available to end preventable stillbirths.
Keywords: Classification; Measurement; Stillbirth; Survey.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Blencowe H, Cousens S, Jassir FB, Say L, Chou D, Mathers C, Hogan D, Shiekh S, Qureshi ZU, You D, Lawn JE. National, regional, and worldwide estimates of stillbirth rates in 2015, with trends from 2000: a systematic analysis. Lancet Glob Health. 2016;4:e98–e108. doi: 10.1016/S2214-109X(15)00275-2. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
