

Termination of pregnancy data completeness and feasibility in population-based surveys: EN-INDEPTH study
- PMID: 33557867
- PMCID: PMC7869447
- DOI: 10.1186/s12963-020-00238-9
Termination of pregnancy data completeness and feasibility in population-based surveys: EN-INDEPTH study
Abstract
Background: Termination of pregnancy (TOP) is a common cause of maternal morbidity and mortality in low- and middle-income countries. Population-based surveys are the major data source for TOP data in LMICs but are known to have shortcomings that require improving. The EN-INDEPTH multi-country survey employed a full pregnancy history approach with roster and new questions on TOP and Menstrual Restoration. This mixed methods paper assesses the completeness of responses to questions eliciting TOP information from respondents and reports on practices, barriers, and facilitators to TOP reporting.
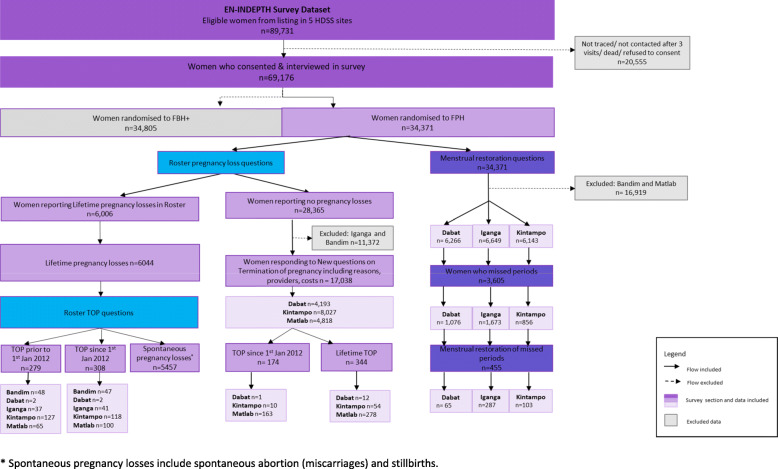
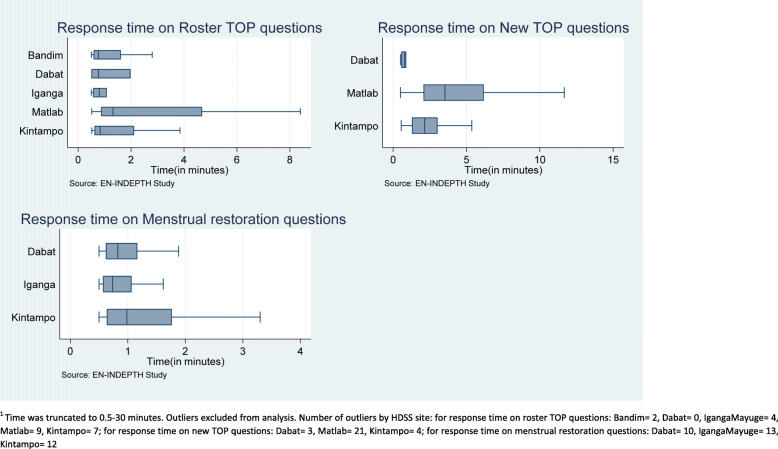
Methods: The EN-INDEPTH study was a population-based cross-sectional study. The Full Pregnancy History arm of the study surveyed 34,371 women of reproductive age between 2017 and 2018 in five Health and Demographic Surveillance System (HDSS) sites of the INDEPTH network: Bandim, Guinea-Bissau; Dabat, Ethiopia; IgangaMayuge, Uganda; Kintampo, Ghana; and Matlab, Bangladesh. Completeness and time spent in answering TOP questions were evaluated using simple tabulations and summary statistics. Exact binomial 95% confidence intervals were computed for TOP rates and ratios. Twenty-eight (28) focus group discussions were undertaken and analysed thematically.
Results: Completeness of responses regarding TOP was between 90.3 and 100.0% for all question types. The new questions elicited between 2.0% (1.0-3.4), 15.5% (13.9-17.3), and 11.5% (8.8-14.7) lifetime TOP cases over the roster questions from Dabat, Ethiopia; Matlab, Bangladesh; and Kintampo, Ghana, respectively. The median response time on the roster TOP questions was below 1.3 minutes in all sites. Qualitative results revealed that TOP was frequently stigmatised and perceived as immoral, inhumane, and shameful. Hence, it was kept secret rendering it difficult and uncomfortable to report. Miscarriages were perceived to be natural, being easier to report than TOP. Interviewer techniques, which were perceived to facilitate TOP disclosure, included cultural competence, knowledge of contextually appropriate terms for TOP, adaptation to interviewee's individual circumstances, being non-judgmental, speaking a common language, and providing detailed informed consent.
Conclusions: Survey roster questions may under-represent true TOP rates, since the new questions elicited responses from women who had not disclosed TOP in the roster questions. Further research is recommended particularly into standardised training and approaches to improving interview context and techniques to facilitate TOP reporting in surveys.
Keywords: Abortion; Completeness; Health and demographic surveillance; Household survey; Population-based surveys; Termination of pregnancy.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Guttmacher Institute . Induced abortion worldwide – global incidence and trends. 2019.
-
- Singh S, Remez L, Sedgh G, Kwok L, Onda T. Abortion worldwide 2017: uneven progress and unequal access; 2018.
-
- Ganatra B, Gerdts C, Rossier C, Johnson BR, Jr, Tunçalp Ö, Assifi A, Sedgh G, Singh S, Bankole A, Popinchalk A. Global, regional, and subregional classification of abortions by safety, 2010–14: estimates from a Bayesian hierarchical model. Lancet. 2017;390:2372–2381. doi: 10.1016/S0140-6736(17)31794-4. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
