

Review
doi: 10.1186/s13054-020-03399-z.
SARS-CoV-2 pneumonia-receptor binding and lung immunopathology: a narrative review
Affiliations
- PMID: 33557908
- PMCID: PMC7870126
- DOI: 10.1186/s13054-020-03399-z
Item in Clipboard
Review
SARS-CoV-2 pneumonia-receptor binding and lung immunopathology: a narrative review
Crit Care.
.
Abstract
The current pandemic of COVID-19 caused thousands of deaths and healthcare professionals struggle to properly manage infected patients. This review summarizes information about SARS-CoV-2 receptor binding dynamics and intricacies, lung autopsy findings, immune response patterns, evidence-based explanations for the immune response, and COVID-19-associated hypercoagulability.
Keywords: ACE2; Acute respiratory distress syndrome; COVID-19; Hypercoagulability; Immunology; Pathology; SARS-CoV-2 pneumonia.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
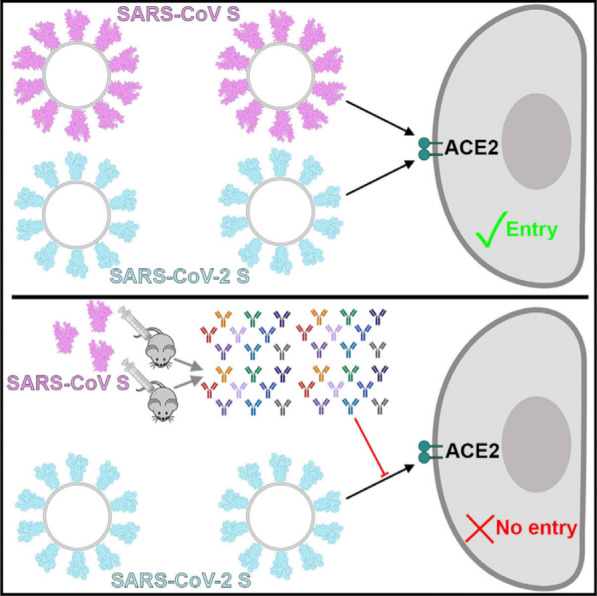
Severe Acute Respiratory Syndrome coronavirus 2 (SARS-CoV-2) binds with high affinity to human angiotensin-converting enzyme 2 (ACE2) and uses it as an entry receptor to invade target cells. Cryo-Electron Microscopy structures of the SARS-CoV-2 spike glycoprotein in two distinct conformations, along with inhibition of spike-mediated entry by SARS-CoV (the coronavirus that emerged in the Guangdong province of China in 2002) polyclonal antibodies, provide a blueprint for the design of vaccines and therapeutics; Permission was granted by Walls et al. (©Elsevier [21]) to reuse this figure
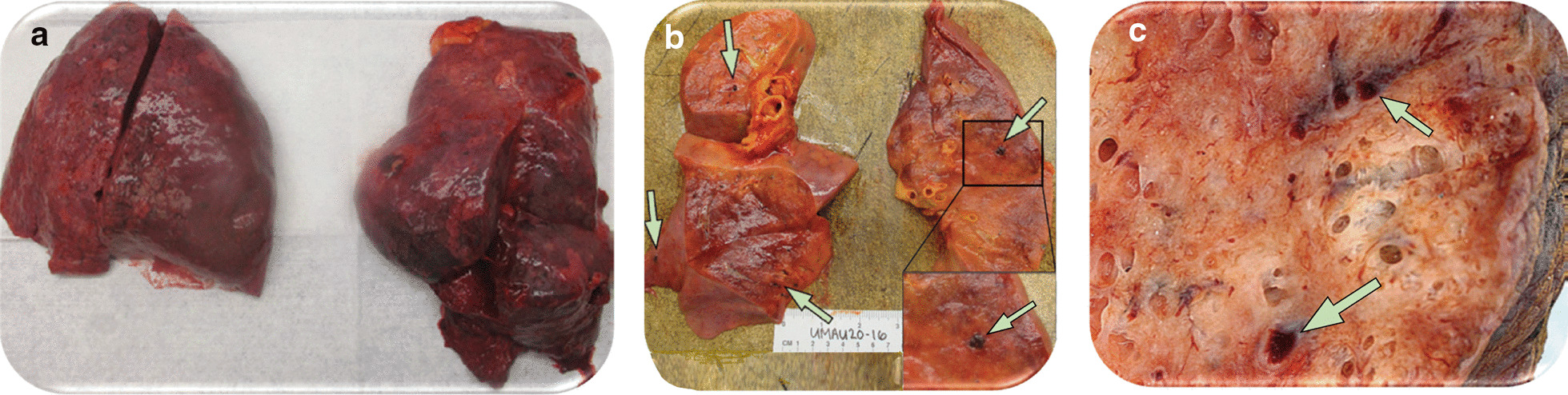
Gross appearance of lungs from two patients who died from severe SARS-CoV-2 pneumonia a Lungs with bilateral pulmonary oedema and patches of dark haemorrhage. b and c Cut sections of lung showing thrombi present within peripheral small vessels (green arrows). Permission was granted by Fox et al. (©Elsevier [28]) to reuse this figure (a and b) and Permission was granted by Ackermann et al. (©Massachusetts Medical Society [29]) to reuse this figure (c)
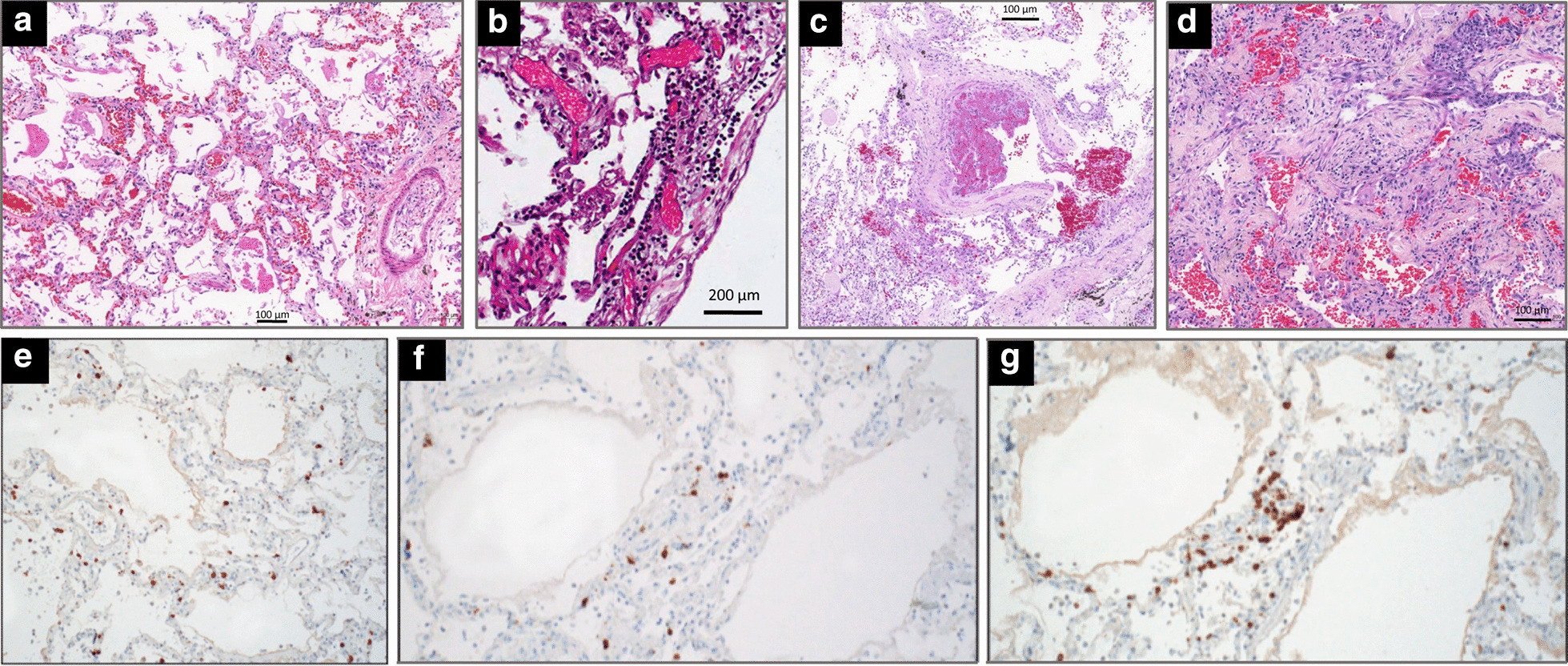
Microscopic findings in the lungs of five patients who died from coronavirus disease 2019. a In a 76-year-old man with hypertension who died from a cardiac arrest 10 days after the onset of symptoms (no admission in the ICU), diffuse alveolar damage with vascular congestion, oedema and perivascular lymphocytic infiltration is present; b In a 78-year-old man with hypertension, morbid obesity, diabetes type 2 who died from hypoxic cardiorespiratory failure three days after hospital admission and two days of non-invasive ventilation, interstitial pneumonia with perivascular lymphocytic infiltration of interalveolar septa and multifocal endothelialitis is present; c In a 63-year-old man without co-morbidity who died from hypoxic cardiorespiratory failure 37 days after onset of symptoms and 26 days after ICU admission and invasive ventilation, partial thrombosis of a pulmonary arteriole with perivascular lymphocytic infiltration is present; d In a 64-year-old man without co-morbidity who died from hypoxic cardiorespiratory failure 21 days after onset of symptoms and 15 days after ICU admission and invasive ventilation, diffuse alveolar damage at a proliferative phase is present with collagen plugs deposition in alveolar spaces (hematoxylin staining collagen in light pink and paucicellular areas); e–g In a 77-year-old man with hypertension and mild obesity, who died on hospital admission six days after onset of symptoms, an interstitial pneumonia is present. T-lymphocytes are highlighted by immunohistochemical stains for CD3 (e), CD4 (f), and CD8 (g). Reproduced from the Department of Pathology of Hospital das Clinicas, Sao Paulo, Brazil (a, c and d) and Permission was granted by Ackermann et al. (©Massachusetts Medical Society [29]) to reuse this figure (b) and Permission was granted by Barton et al. (©Oxford University Press [31]) to reuse this figure (e–f)
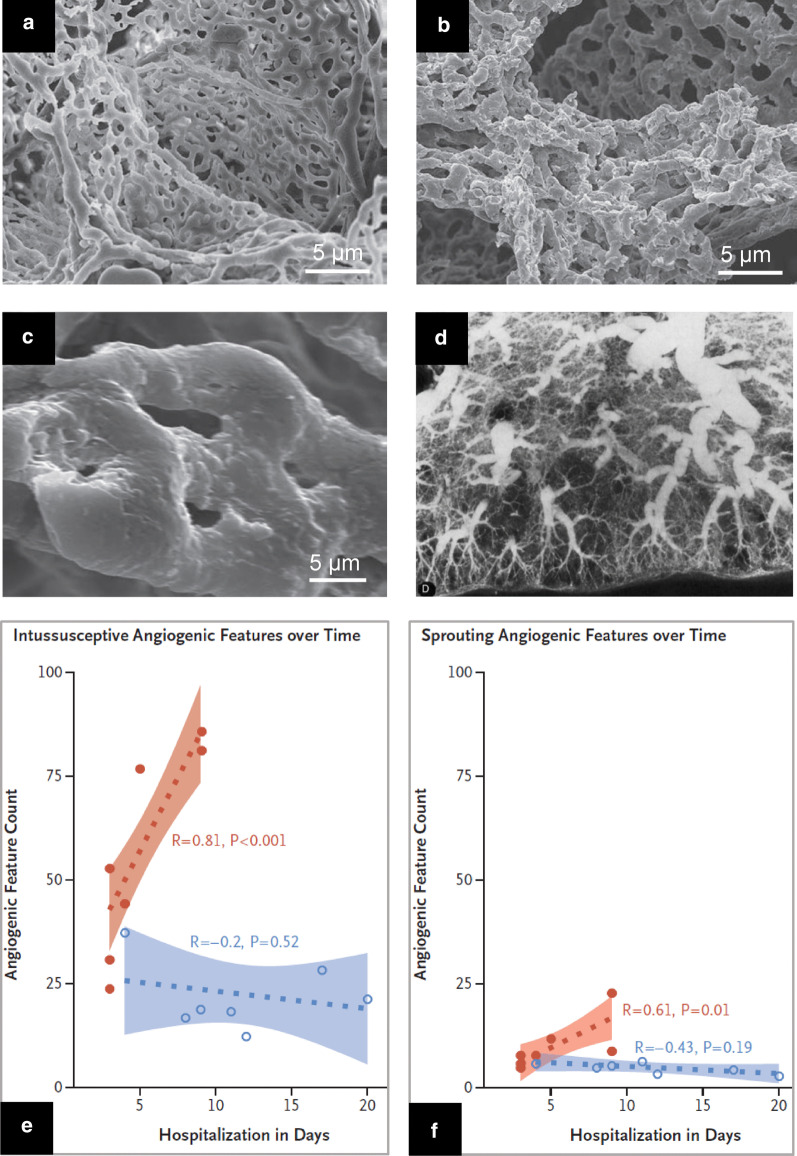
Angiogenesis and neovascularization in patients with severe SARS-CoV-2 pneumonia a Electron microcopy showing microvascular corrosion casts from the alveolar plexus of a healthy lung b Electron microcopy showing microvascular corrosion casts from the alveolar plexus of a COVID-19 injured lung with substantial architectural distortion c Electron microscopy showing pillar localizations (arrowheads) associated with the intussusceptive angiogenesis d Postmortem pulmonary arteriogram performed in a patient who died from non-COVID ARDS, 26 days after a massive aspiration. The vascular bed is rarefied and tortuous, suggesting a distorted neovascularization (e and f) Chronological comparison of intussusceptive and sprouting angiogenesis in lungs from patients with Covid-19 (orange colour) and lungs from patients with influenza A(H1N1) (blue colour) plotted as a function of the duration of hospitalization. In COVID 19 patients, intussusceptive angiogenesis predominates over sprouting angiogenesis and markedly increases with time. Permission was granted by Ackermann et al. (©Massachusetts Medical Society [29]) to reuse this figure (a–c, e, f), and Permission was granted by Tomashefski (©Elsevier [39]) to reuse this figure (d)
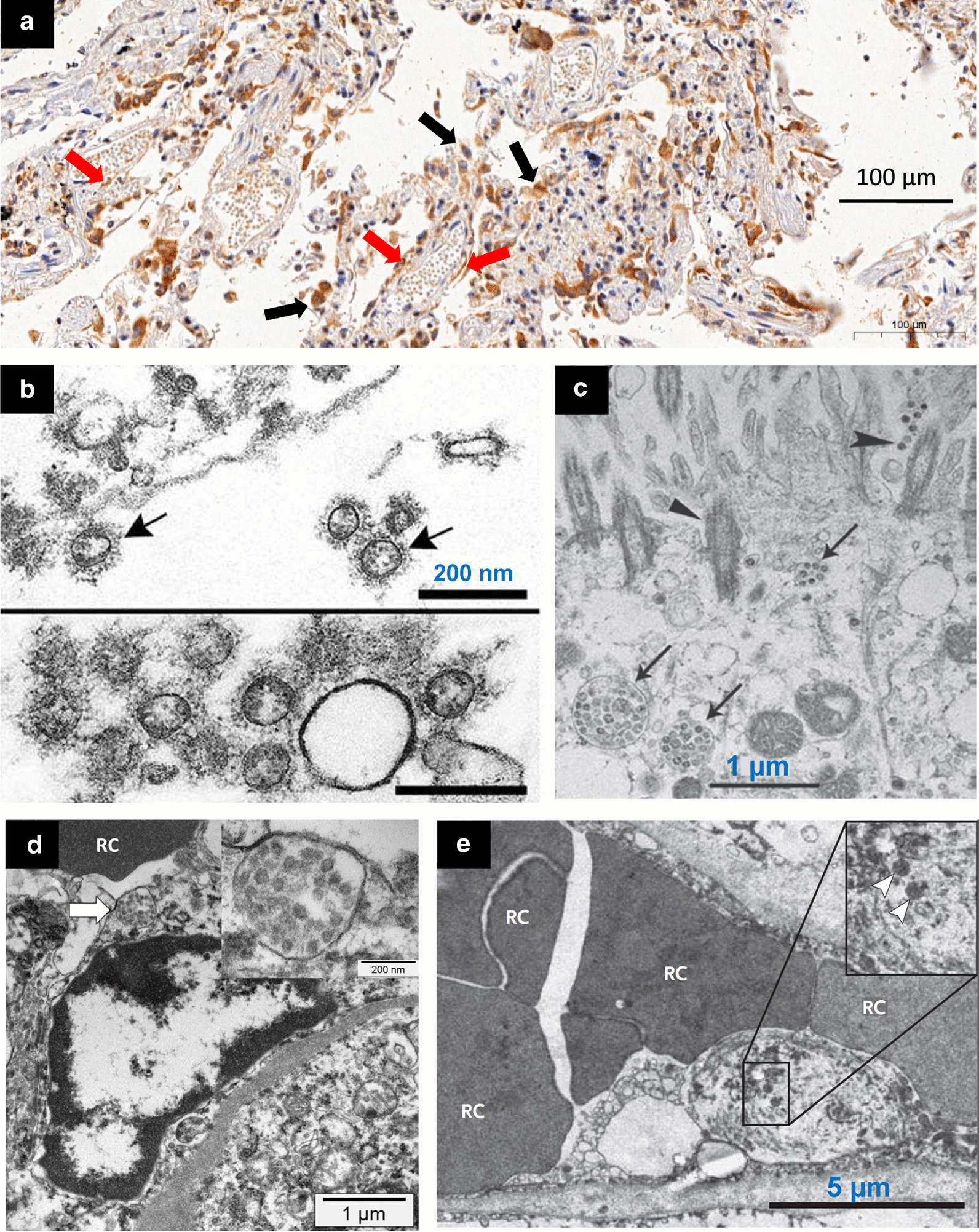
Microscopic histology and electron microscopy showing SARS-CoV-2 in lungs and kidneys of patients who died from COVID 19. a In a 76-year-old man with hypertension who died from a cardiac arrest 10 days after the onset of COVID 19 symptoms (no admission in the ICU), positive immunohistochemistry staining for SARS-CoV-2 is present in lung epithelial cells (black arrows) and endothelial cells (red arrows). Immunostaining was performed using a house-made antibody (University of Sao Paulo, Institute of Biomedical Sciences), using a 1:50 dilution, and revealed with 3,3′-Diaminobenzidine staining system b Alveolar space containing extracellular SARS-CoV-2 (arrows) with prominent surface profections (bottom: cluster of virions) c Extracellular SARS-CoV-2 particles (arrows) present in the airway epithelial and cilia (triangles). d An activated glomerular endothelial cell containing a vesicle close to the luminal border with virus-like particles (arrow and insert), adjacent to an erythrocyte (RC). e Injured endothelial cell of a pulmonary capillary containing SARS-CoV-2 (arrowheads). Swelling of the nucleus and cytoplasm partially obstructs the capillary lumen. Permission was granted by Martines et al. (©Centers for Disease Control and Prevention [38]) to reuse this figure (b), Permission was granted by Zhu et al. (©Massachusetts Medical Society [2]) to reuse this figure (c), Permission was granted by Menter et al. (©Public License (Creative Commons) [35]) to reuse this figure (d) and Permission was granted by Ackermann et al. (©The New England Journal of Medicine [29]) to reuse this figure (e)
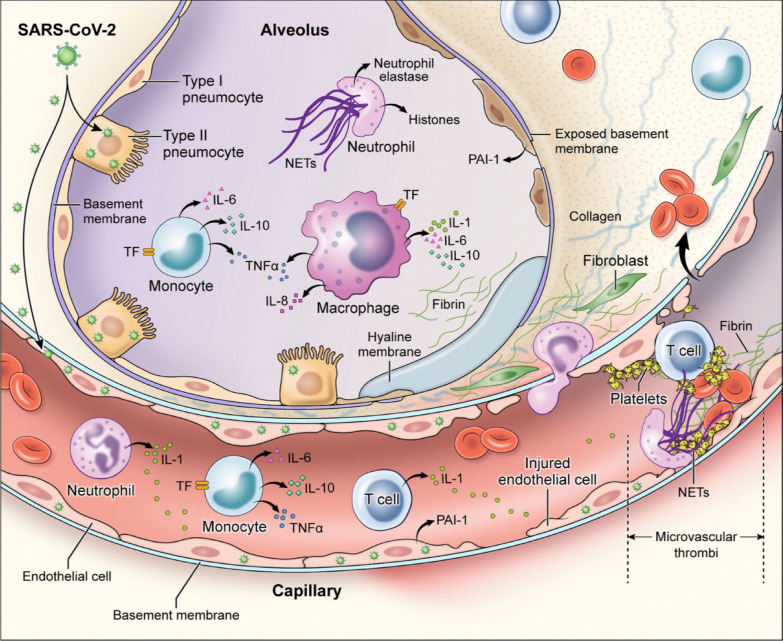
Mechanisms of coagulopathy in patients with SARS-CoV-2 pneumonia: direct infection of type II pneumocytes and endothelial cells, leading to increased barrier permeability; inflammatory activation of T cells, neutrophils, monocytes, macrophages, and platelets resulting in exuberant inflammatory cytokine release, monocyte-derived TF and PAI-1 expression; development of microvascular and macrovascular thrombi composed of fibrin, NETs, and platelets. IL = interleukin; NETs = neutrophil extracellular traps; PAI-1 = plasminogen activator inhibitor-1; TF = tissue factor; TNF-α = tumor necrosis factor-alpha. Permission was granted by Colling and Kanthi (©Public License (Creative Commons) [82]) to reuse this figure
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
