

Effects of COVID-19 on in-hospital cardiac arrest: incidence, causes, and outcome - a retrospective cohort study
- PMID: 33557923
- PMCID: PMC7868866
- DOI: 10.1186/s13049-021-00846-w
Effects of COVID-19 on in-hospital cardiac arrest: incidence, causes, and outcome - a retrospective cohort study
Abstract
Background: Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), an emerging virus, has caused a global pandemic. Coronavirus disease 2019 (COVID-19), caused by SARS-CoV-2, has led to high hospitalization rates worldwide. Little is known about the occurrence of in-hospital cardiac arrest (IHCA) and high mortality rates have been proposed. The aim of this study was to investigate the incidence, characteristics and outcome of IHCA during the pandemic in comparison to an earlier period.
Methods: This was a retrospective analysis of data prospectively recorded during 3-month-periods 2019 and 2020 at the University Medical Centre Hamburg-Eppendorf (Germany). All consecutive adult patients with IHCA were included. Clinical parameters, neurological outcomes and organ failure/support were assessed.
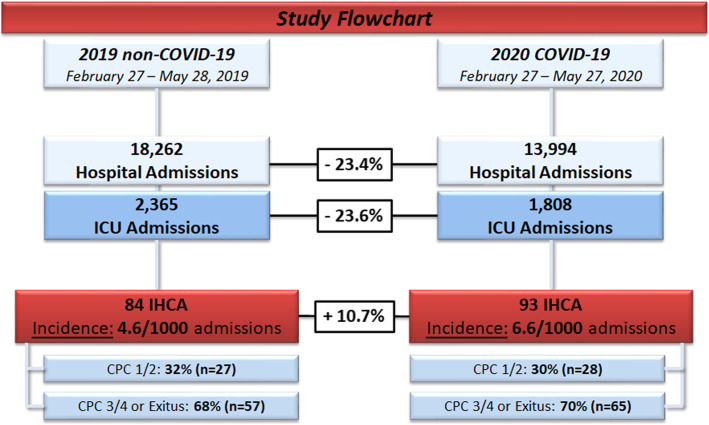
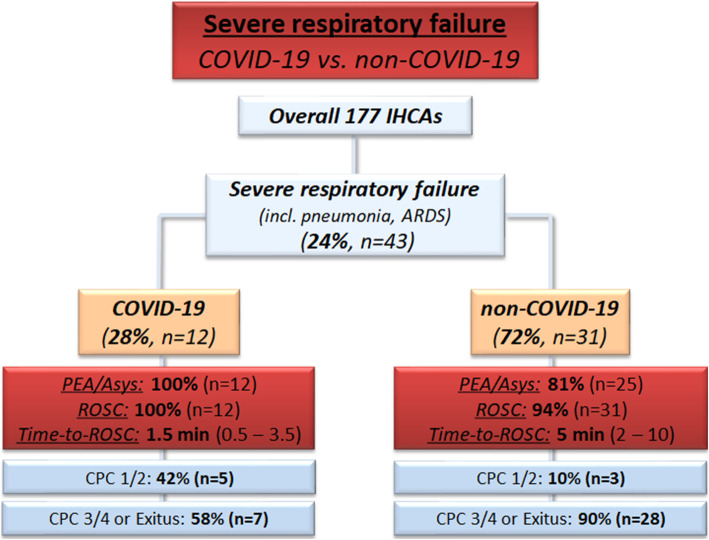
Results: During the study period hospital admissions declined from 18,262 (2019) to 13,994 (2020) (- 23%). The IHCA incidence increased from 4.6 (2019: 84 IHCA cases) to 6.6 (2020: 93 IHCA cases)/1000 hospital admissions. Median stay before IHCA was 4 (1-9) days. Demographic characteristics were comparable in both periods. IHCA location shifted towards the ICU (56% vs 37%, p < 0.01); shockable rhythm (VT/VF) (18% vs 29%, p = 0.05) and defibrillation were more frequent in the pandemic period (20% vs 35%, p < 0.05). Resuscitation times, rates of ROSC and post-CA characteristics were comparable in both periods. The severity of illness (SAPS II/SOFA), frequency of mechanical ventilation and frequency of vasopressor therapy after IHCA were higher during the 2020 period. Overall, 43 patients (12 with & 31 without COVID-19), presented with respiratory failure at the time of IHCA. The Horowitz index and resuscitation time were significantly lower in patients with COVID-19 (each p < 0.01). Favourable outcomes were observed in 42 and 10% of patients with and without COVID-19-related respiratory failure, respectively.
Conclusion: Hospital admissions declined during the pandemic, but a higher incidence of IHCA was observed. IHCA in patients with COVID-19 was a common finding. Compared to patients with non-COVID-19-related respiratory failure, the outcome was improved.
Keywords: COVID-19; Cardiac arrest; Cardiopulmonary resuscitation; Corona virus disease; In-hospital cardiac arrest; Intensive care unit; Multiple organ failure; SARS-COV-2.
Conflict of interest statement
KR, GS, DF, JM, MI, DW and DJ do not report any conflicts of interest related to this article. SK received research support by Ambu, E.T.View Ltd., Fisher & Paykel, Pfizer and Xenios, lecture honorarium from ArjoHuntleigh, Astellas, Astra, Basilea, Bard, Baxter, Biotest, CSL Behring, Cytosorbents, Fresenius, Gilead, MSD, Orion, Pfizer, Philips, Sedana, Sorin, Xenios and Zoll, and consultant honorarium from AMOMED, Astellas, Baxter, Bayer, Fresenius, Gilead, MSD, Pfizer and Xenios. No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Letter to the Editor in regard to the "Effects of COVID-19 on in-hospital cardiac arrest: incidence, causes, and outcome" by Roedl et al.".Scand J Trauma Resusc Emerg Med. 2021 Nov 3;29(1):159. doi: 10.1186/s13049-021-00965-4. Scand J Trauma Resusc Emerg Med. 2021. PMID: 34732229 Free PMC article. No abstract available.
References
-
- WHO. WHO - World Map - COVID-19. 2020 [https://covid19.who.int/ - Accessed online: October, 31st 2020] [Available from: https://covid19.who.int/ - Accessed online: October, 19th 2020].
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
