

Grave thoraco-intestinal complication secondary to an undetected traumatic rupture of the diaphragm: a case report
- PMID: 33557953
- PMCID: PMC7871382
- DOI: 10.1186/s40001-021-00488-9
Grave thoraco-intestinal complication secondary to an undetected traumatic rupture of the diaphragm: a case report
Abstract
Background: Diaphragmatic lesions as a result of blunt or penetrating trauma are challenging to detect in the initial trauma setting. This is especially true when diaphragmatic trauma is part of a polytrauma. Complications of undetected diaphragmatic defects with incarcerating bowel are rare, but as in our patient can be serious.
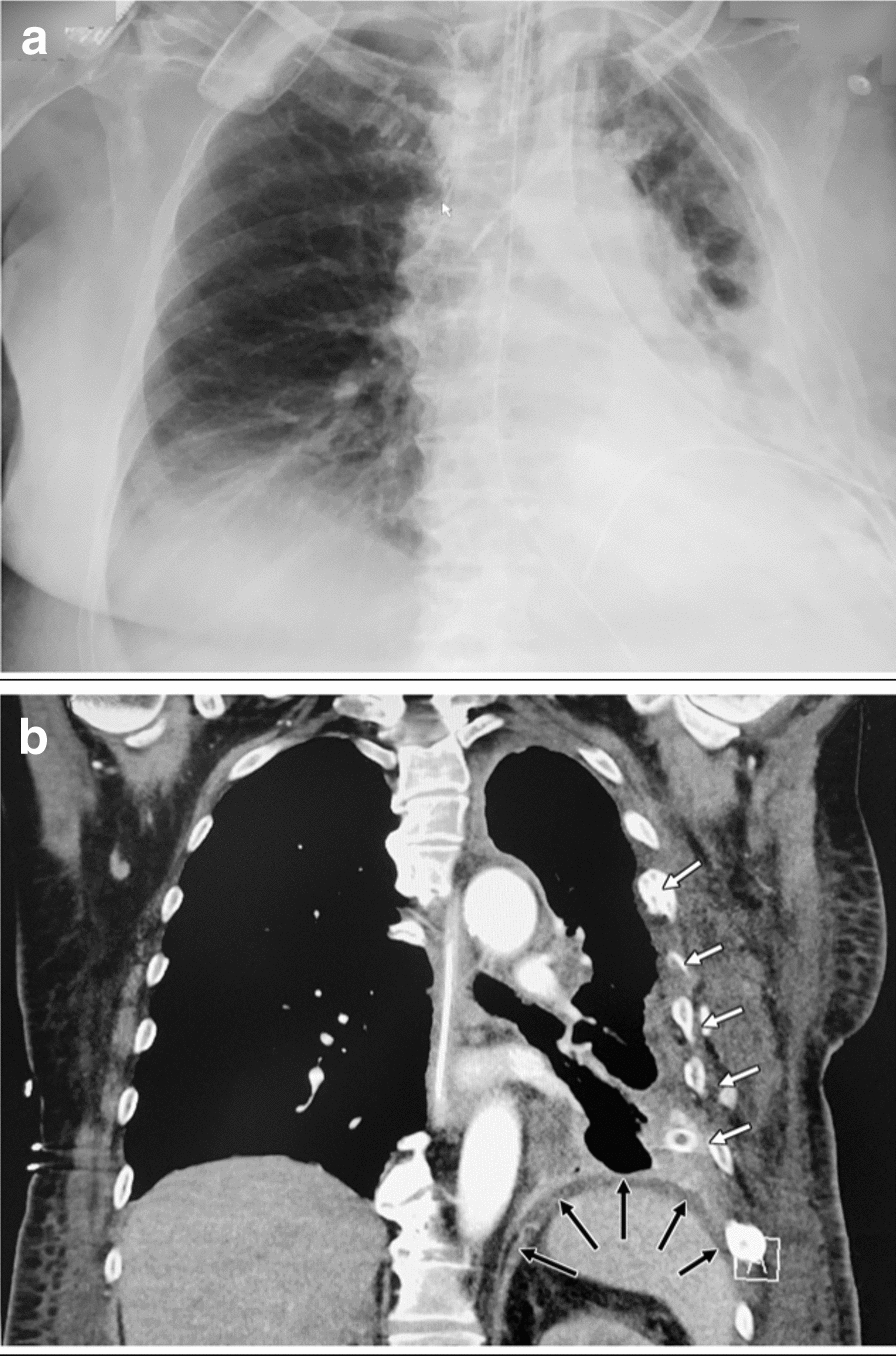
Case presentation: A 57-year-old female presented to the Emergency Room of our Hospital in a critical condition with 3 days of increasing abdominal pain. The initial clinical examination showed peritonism with tinkling peristaltic bowel sounds of mechanical obstruction. A thoraco-abdominal CT scan demonstrated colon prolapsed through the left diaphragmatic center with a large sero-pneumothorax under tension. As the patient was hemodynamically increasingly unstable with developing septic shock, an emergency laparotomy was performed. After retraction of the left colon, which had herniated through a defect of the tendinous center of the left diaphragm and was perforated due to transmural ischemia, large amounts of feces and gas discharged from the left thorax. A left hemicolectomy resulting in a Hartmann-type procedure was performed. A fully established pleural empyema required meticulous debridement and lavage conducted via the 7-10 cm in diameter phrenic opening followed by a diaphragmatic defect reconstruction. Due to pneumonia and recurring pleural empyema redo-debridement of the left pleural space via thoracotomy were required. The patient was discharged on day 56. A thorough history of possible trauma revealed a bicycle-fall trauma 7 months prior to this hospitalization with a surgically stabilized fracture of the left femur and conservatively treated fractures of ribs 3-9 on the left side.
Conclusion: This is the first report on a primarily established empyema at the time of first surgical intervention for feco-pneumothorax secondary to delayed diagnosed diaphragmatic rupture following abdomino-thoracic blunt trauma with colic perforation into the pleural space, requiring repetitive surgical debridement in order to control local and systemic sepsis. Thorough investigation should always be undertaken in cases of blunt abdominal and thoracic trauma to exclude diaphragmatic injury in order to avoid post-traumatic complications.
Keywords: Bowel perforation; Case report; Diaphragmatic rupture; Herniation; Pleural empyema; Pneumothorax.
Conflict of interest statement
No competing interests or conflicts exist for any author to declare.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
