

Genomic Analysis of Circulating Tumor DNA in 3,334 Patients with Advanced Prostate Cancer Identifies Targetable BRCA Alterations and AR Resistance Mechanisms
- PMID: 33558422
- PMCID: PMC9295199
- DOI: 10.1158/1078-0432.CCR-20-4805
Genomic Analysis of Circulating Tumor DNA in 3,334 Patients with Advanced Prostate Cancer Identifies Targetable BRCA Alterations and AR Resistance Mechanisms
Abstract
Purpose: Comprehensive genomic profiling (CGP) is of increasing value for patients with metastatic castration-resistant prostate cancer (mCRPC). mCRPC tends to metastasize to bone, making tissue biopsies challenging to obtain. We hypothesized CGP of cell-free circulating tumor DNA (ctDNA) could offer a minimally invasive alternative to detect targetable genomic alterations (GA) that inform clinical care.
Experimental design: Using plasma from 3,334 patients with mCRPC (including 1,674 screening samples from TRITON2/3), we evaluated the landscape of GAs detected in ctDNA and assessed concordance with tissue-based CGP.
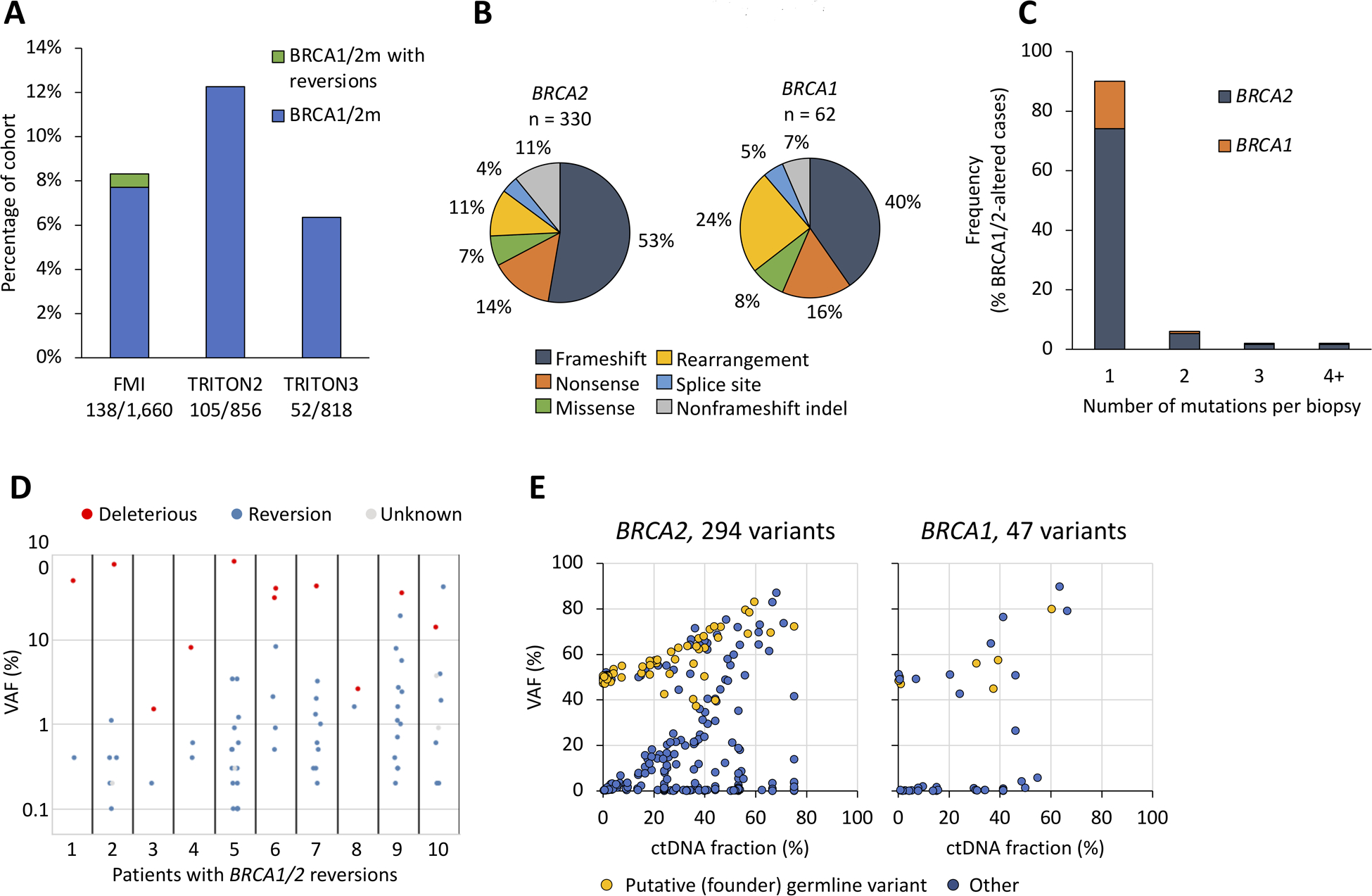
Results: A total of 3,129 patients (94%) had detectable ctDNA with a median ctDNA fraction of 7.5%; BRCA1/2 was mutated in 295 (8.8%). In concordance analysis, 72 of 837 patients had BRCA1/2 mutations detected in tissue, 67 (93%) of which were also identified using ctDNA, including 100% of predicted germline variants. ctDNA harbored some BRCA1/2 alterations not identified by tissue testing, and ctDNA was enriched in therapy resistance alterations, as well as possible clonal hematopoiesis mutations (e.g., in ATM and CHEK2). Potential androgen receptor resistance alterations were detected in 940 of 2,213 patients (42%), including amplifications, polyclonal and compound mutations, rearrangements, and novel deletions in exon 8.
Conclusions: Genomic analysis of ctDNA from patients with mCRPC recapitulates the genomic landscape detected in tissue biopsies, with a high level of agreement in detection of BRCA1/2 mutations, but more acquired resistance alterations detected in ctDNA. CGP of ctDNA is a compelling clinical complement to tissue CGP, with reflex to tissue CGP if negative for actionable variants.See related commentary by Hawkey and Armstrong, p. 2961.
©2021 American Association for Cancer Research.
Conflict of interest statement
Disclosure of Potential Conflicts of Interest:
COI: HT, RWM, JHC, EAS, LD, BJF, SM, LZ, RPG, JSR, BMA, JMV, and GRO are employees of Foundation Medicine, a wholly owned subsidiary of Roche, and have equity interest in Roche. TG, SPW, AS, and AL are employees of Clovis Oncology. WA has served as consultant or advisor to or received travel, accommodations or expenses from Clovis Oncology, Daiichi Sankyo, Glaxo-Kline Smith, Janssen, MORE Health and ORIC Pharmaceuticals. CJR has received honoraria or served as consultant or advisor to Advanced Accelerator Applications, Bayer, Bristol Myers Squibb, Dendreon, Janssen Oncology, Myovant Sciences, and Roivant. KF has received honoraria and travel, accommodations or expenses from, or served as consultant or advisor to, Astellas Pharma, Bayer, Curevac, Janssen Oncology, Orion Pharma GmbH, and Sanofi. SC has received honoraria from, served as consultant or advisor to, or is part of the Speaker’ Bureau for Astellas Pharma, Bayer, BeiGene, Clovis Oncology, Janssen-Cilag, Novartis, and Pfizer.
Figures



Comment in
-
Building confidence in circulating tumour DNA assays for metastatic castration-resistant prostate cancer.Nat Rev Urol. 2021 May;18(5):255-256. doi: 10.1038/s41585-021-00455-3. Nat Rev Urol. 2021. PMID: 33742188 No abstract available.
-
Liquid Biopsy: It's the Bloody Truth!Clin Cancer Res. 2021 Jun 1;27(11):2961-2963. doi: 10.1158/1078-0432.CCR-21-0531. Epub 2021 Apr 1. Clin Cancer Res. 2021. PMID: 33795259 Free PMC article.
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians. 2018; 68: 394–424. - PubMed
-
- Nuhn P, de Bono JS, Fizazi K, Freedland SJ, Grilli M, Kantoff PW, et al. Update on Systemic Prostate Cancer Therapies: Management of Metastatic Castration-resistant Prostate Cancer in the Era of Precision Oncology [Internet]. European Urology. 2019. page 88–99. - PubMed
-
- de Wit R, de Bono J, Sternberg CN, Fizazi K, Tombal B, Wülfing C, et al. Cabazitaxel versus Abiraterone or Enzalutamide in Metastatic Prostate Cancer. New England Journal of Medicine. 2019; 381: 2506–18. - PubMed
-
- Oh WK, Cheng WY, Miao R, Vekeman F, Gauthier-Loiselle M, Duh MS, et al. Real-world outcomes in patients with metastatic castration-resistant prostate cancer receiving second-line chemotherapy versus an alternative androgen receptor-targeted agent (ARTA) following early progression on a first-line ARTA in a US community oncology setting. Urologic Oncology: Seminars and Original Investigations. 2018; 36: 500.e1–500.e9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
