

Modeling the effect of lockdown timing as a COVID-19 control measure in countries with differing social contacts
- PMID: 33558571
- PMCID: PMC7870675
- DOI: 10.1038/s41598-021-82873-2
Modeling the effect of lockdown timing as a COVID-19 control measure in countries with differing social contacts
Abstract
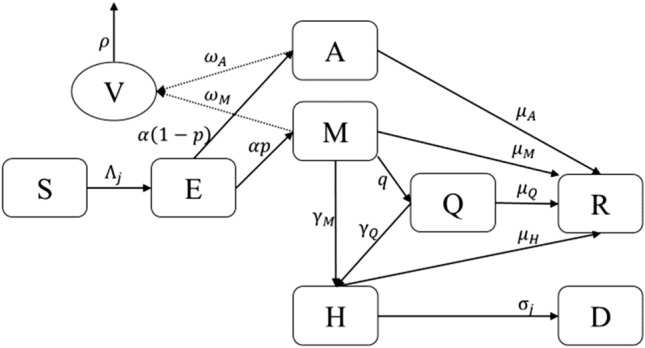
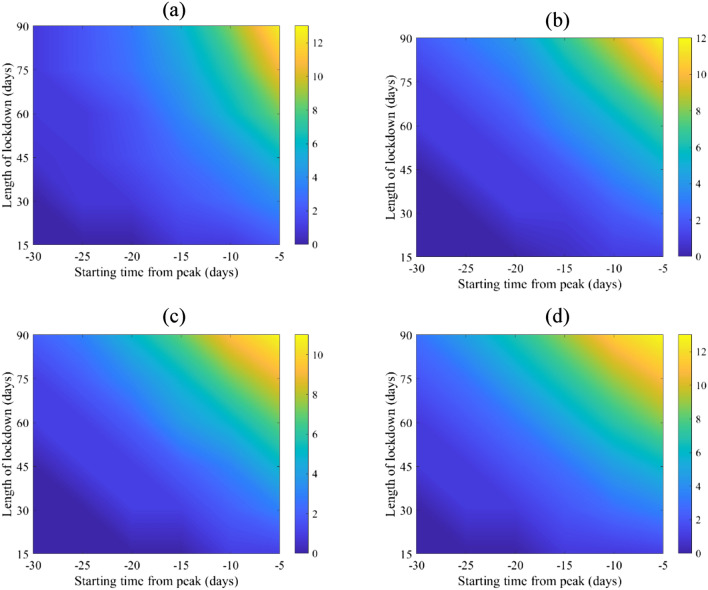
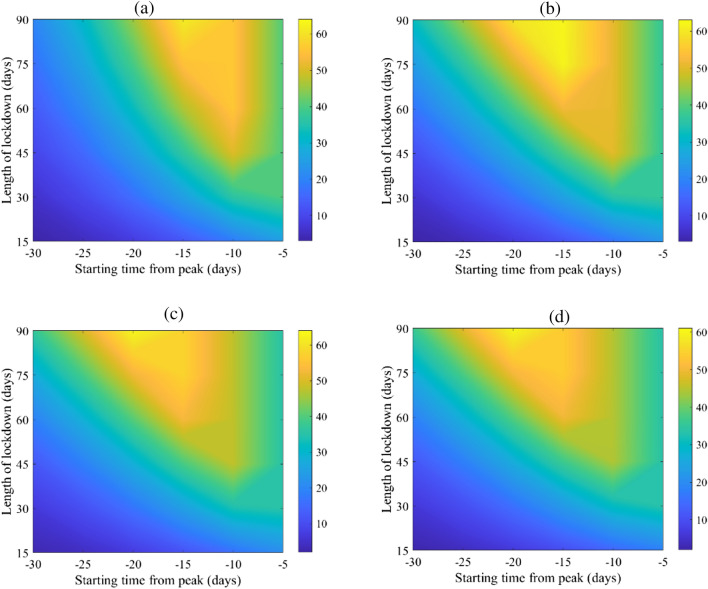
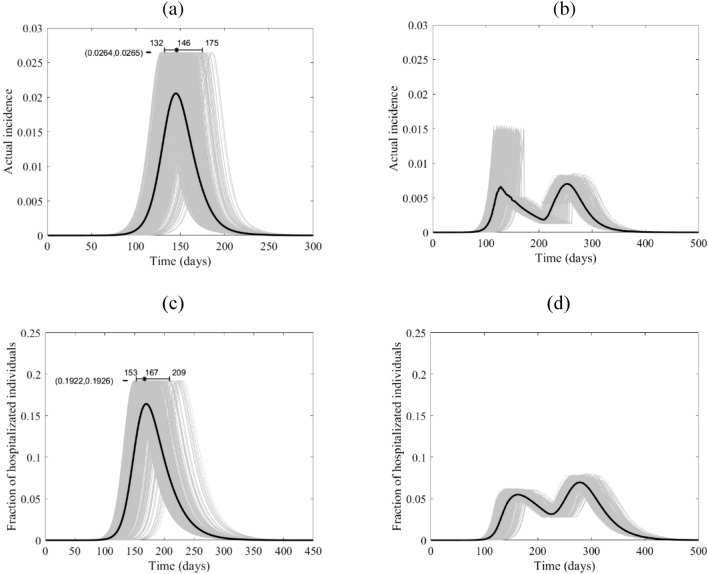
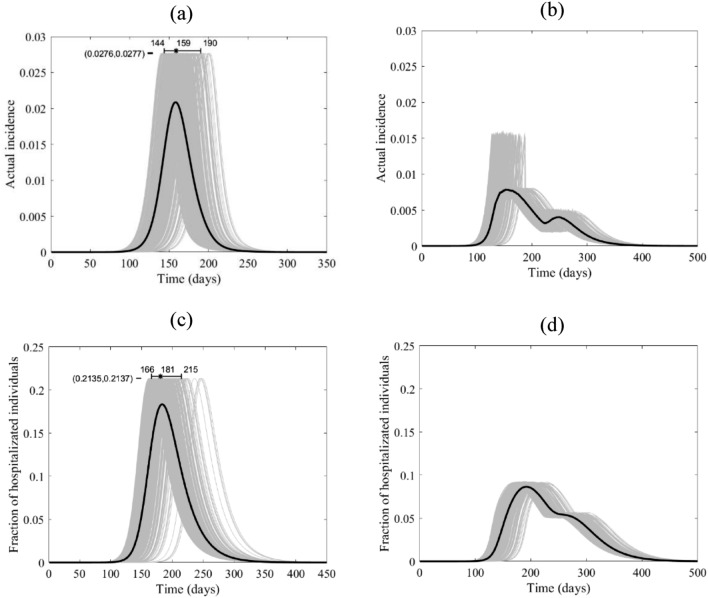
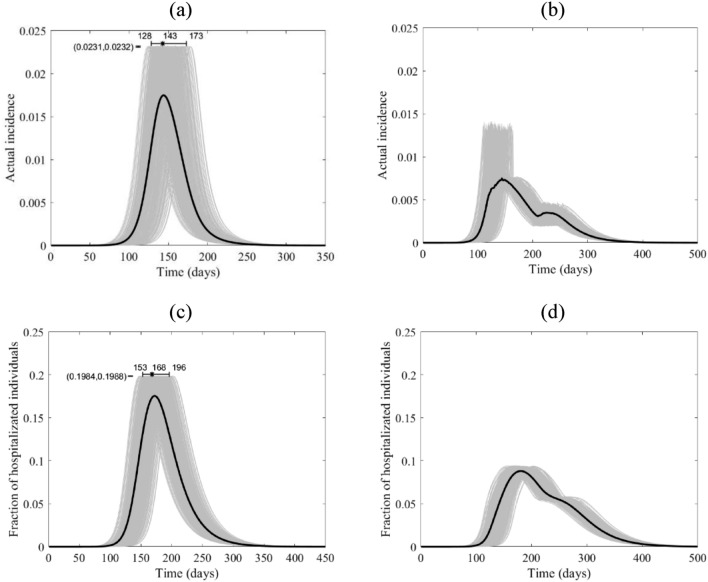
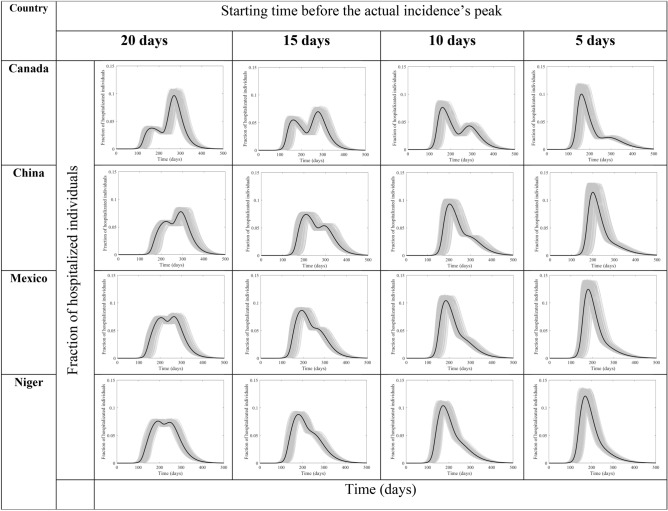
The application, timing, and duration of lockdown strategies during a pandemic remain poorly quantified with regards to expected public health outcomes. Previous projection models have reached conflicting conclusions about the effect of complete lockdowns on COVID-19 outcomes. We developed a stochastic continuous-time Markov chain (CTMC) model with eight states including the environment (SEAMHQRD-V), and derived a formula for the basic reproduction number, R0, for that model. Applying the [Formula: see text] formula as a function in previously-published social contact matrices from 152 countries, we produced the distribution and four categories of possible [Formula: see text] for the 152 countries and chose one country from each quarter as a representative for four social contact categories (Canada, China, Mexico, and Niger). The model was then used to predict the effects of lockdown timing in those four categories through the representative countries. The analysis for the effect of a lockdown was performed without the influence of the other control measures, like social distancing and mask wearing, to quantify its absolute effect. Hypothetical lockdown timing was shown to be the critical parameter in ameliorating pandemic peak incidence. More importantly, we found that well-timed lockdowns can split the peak of hospitalizations into two smaller distant peaks while extending the overall pandemic duration. The timing of lockdowns reveals that a "tunneling" effect on incidence can be achieved to bypass the peak and prevent pandemic caseloads from exceeding hospital capacity.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Majumder, M. & Mandl, K. Early Transmissibility Assessment of a Novel Coronavirus in Wuhan, China (January 26, 2020). https://ssrn.com/abstract=3524675 or 10.2139/ssrn.3524675.
-
- World Health Organization. Statement on Novel Coronavirus in Thailand. Jan 13, 2020. https://www.who.int/news-room/detail/13-01-2020-who-statement-on-novel-c....
-
- World Health Organization. Statement on the second meeting of the International Health Regulations (2005) Emergency Committee regarding the outbreak of novel coronavirus (2019-nCoV). Jan 30, 2020. https://www.who.int/news-room/detail/30-01-2020-statement-on-the-second-...) (2020).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
