

Determination of breast cancer prognosis after neoadjuvant chemotherapy: comparison of Residual Cancer Burden (RCB) and Neo-Bioscore
- PMID: 33558711
- PMCID: PMC8039034
- DOI: 10.1038/s41416-020-01251-3
Determination of breast cancer prognosis after neoadjuvant chemotherapy: comparison of Residual Cancer Burden (RCB) and Neo-Bioscore
Abstract
Background: To compare RCB (Residual Cancer Burden) and Neo-Bioscore in terms of prognostic performance and see if adding pathological variables improve these scores.
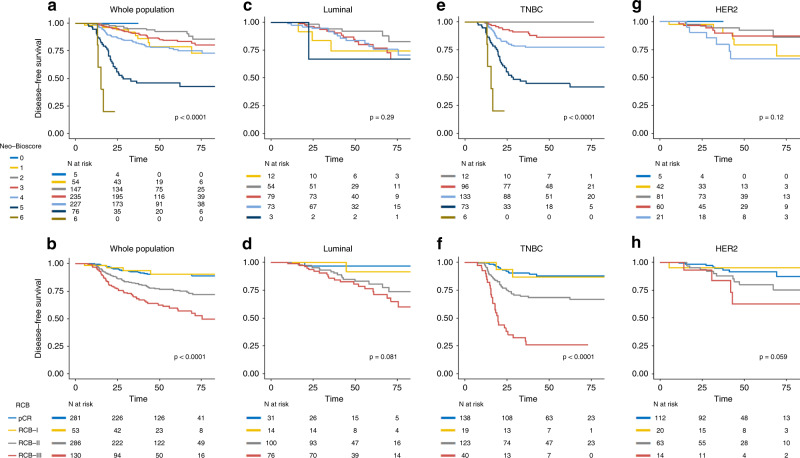
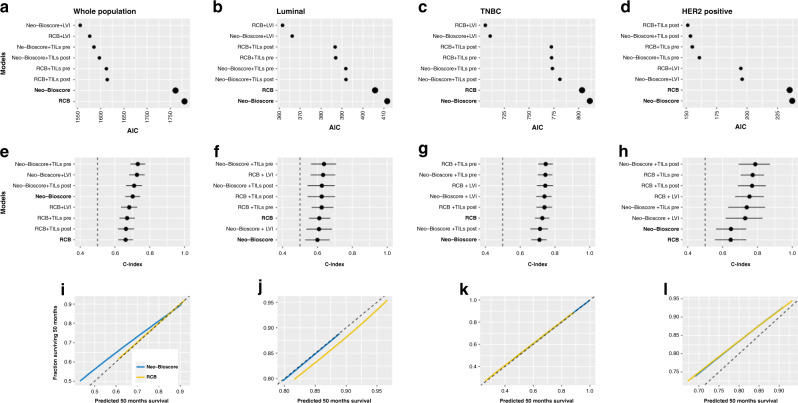
Methods: We analysed 750 female patients with invasive breast cancer (BC) treated with neoadjuvant chemotherapy (NAC) at Institut Curie between 2002 and 2012. Scores were compared in global population and by BC subtype using Akaike information criterion (AIC), C-Index (concordance index), calibration curves and after adding lymphovascular invasion (LVI) and pre-/post-NAC TILs levels.
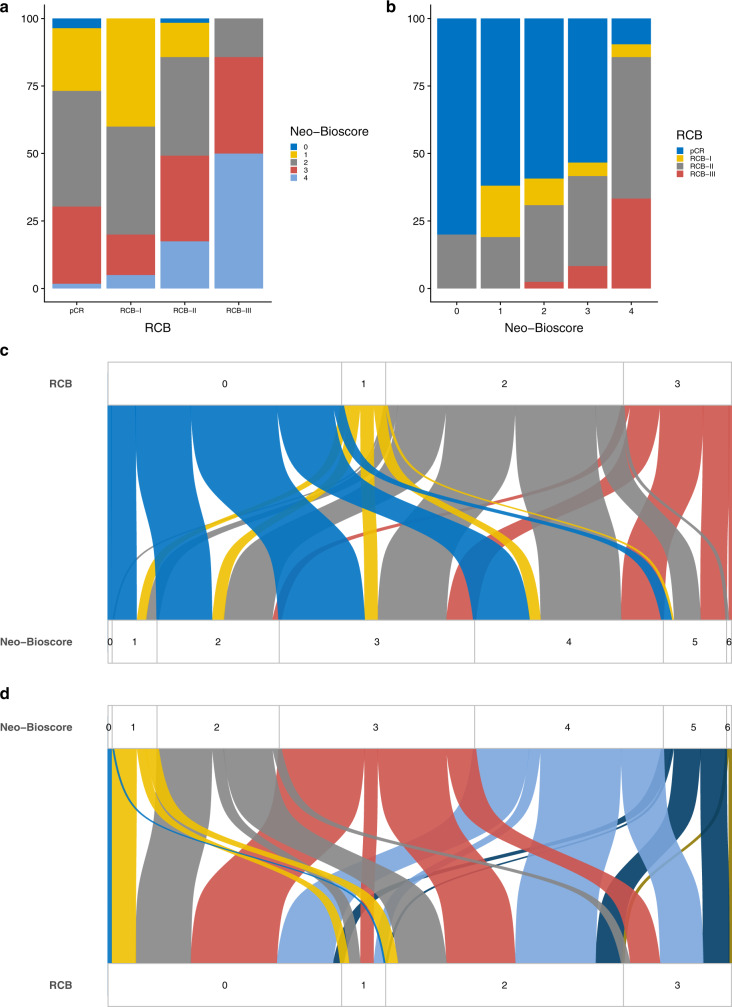
Results: RCB and Neo-Bioscore were significantly associated to disease-free and overall survival in global population and for triple-negative BC. RCB had the lowest AICs in every BC subtype, corresponding to a better prognostic performance. In global population, C-Index values were poor for RCB (0.66; CI [0.61-0.71]) and fair for Neo-Bioscore (0.70; CI [0.65-0.75]). Scores were well calibrated in global population, but RCB yielded better prognostic performances in each BC subtype. Concordance between the two scores was poor. Adding LVI and TILs improved the performance of both scores.
Conclusions: Although RCB and Neo-Bioscore had similar prognostic performances, RCB showed better performance in BC subtypes, especially in luminal and TNBC. By generating fewer prognostic categories, RCB enables an easier use in everyday clinical practice.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Kaufmann M, von Minckwitz G, Bear HD, Buzdar A, McGale P, Bonnefoi H, et al. Recommendations from an international expert panel on the use of neoadjuvant (primary) systemic treatment of operable breast cancer: new perspectives 2006. Ann. Oncol. 2007;18:1927–1934. doi: 10.1093/annonc/mdm201. - DOI - PubMed
-
- Jackisch C, Harbeck N, Huober J, von Minckwitz G, Gerber B, Kreipe H-H, et al. 14th St. Gallen International Breast Cancer Conference 2015: Evidence, Controversies, Consensus—Primary Therapy of Early Breast Cancer: Opinions Expressed by German Experts. Breast Care Basel Switz. 2015;10:211–219. doi: 10.1159/000433590. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
