

How much oxygen for the injured brain - can invasive parenchymal catheters help?
- PMID: 33560016
- PMCID: PMC7987136
- DOI: 10.1097/MCC.0000000000000810
How much oxygen for the injured brain - can invasive parenchymal catheters help?
Abstract
Purpose of review: Each year in the United States there are over 2.5 million visits to emergency departments for traumatic brain injury (TBI), 300,000 hospitalizations, and 50,000 deaths. TBI initiates a complex cascade of events which can lead to significant secondary brain damage. Great interest exists in directly measuring cerebral oxygen delivery and demand after TBI to prevent this secondary injury. Several invasive, catheter-based devices are now available which directly monitor the partial pressure of oxygen in brain tissue (PbtO2), yet significant equipoise exists regarding their clinical use in severe TBI.
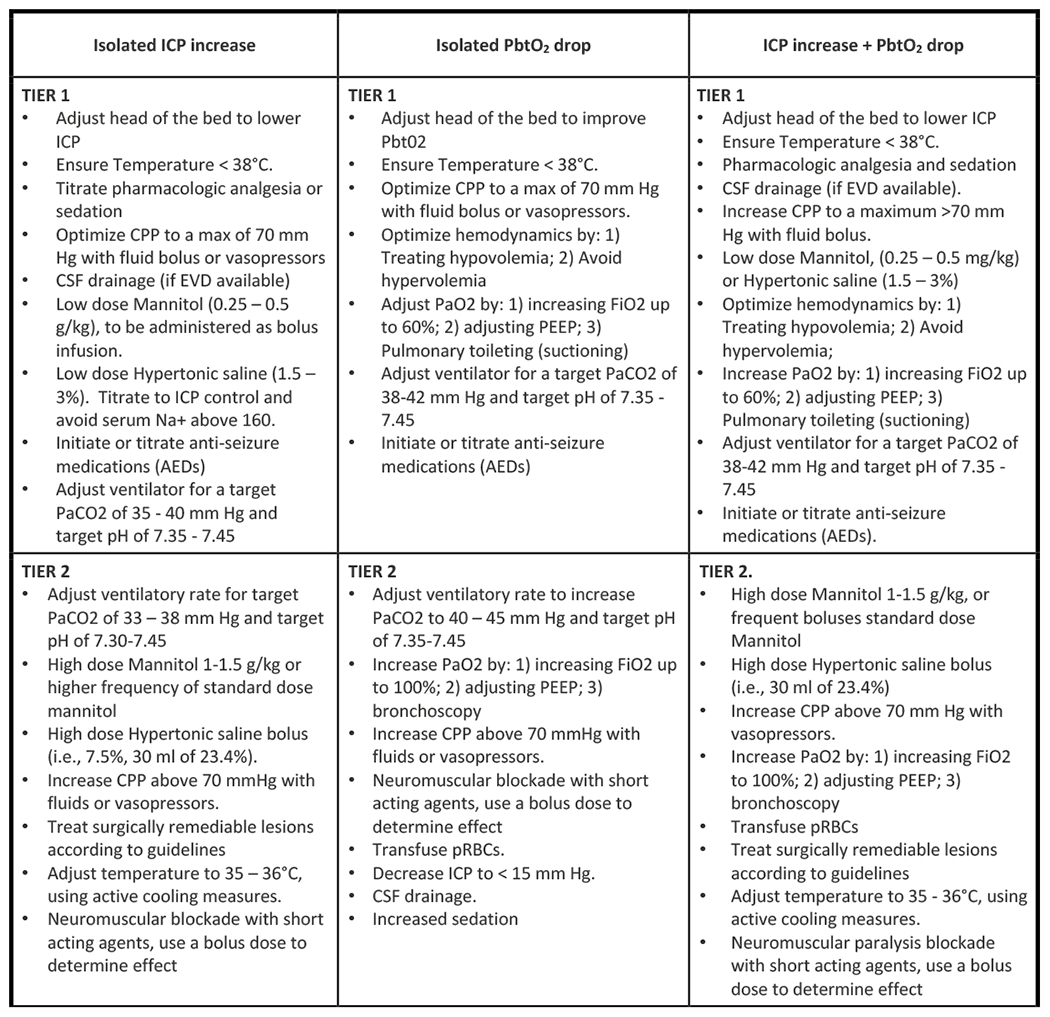
Recent findings: There are currently three ongoing multicenter randomized controlled trials studying the use of PbtO2 monitoring in severe TBI: BOOST-3, OXY-TC, and BONANZA. All three have similar inclusion/exclusion criteria, treatment protocols, and outcome measures. Despite mixed existing evidence, use of PbtO2 is already making its way into new TBI guidelines such as the recent Seattle International Brain Injury Consensus Conference. Analysis of high-fidelity data from multimodal monitoring, however, suggests that PbtO2 may only be one piece of the puzzle in severe TBI.
Summary: While current evidence regarding the use of PbtO2 remains mixed, three ongoing clinical trials are expected to definitively answer the question of what role PbtO2 monitoring plays in severe TBI.
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Conflicts of Interests: Dr. Shutter is one of the principle investigators for BOOST-3, an ongoing randomized controlled trial investigating the use of PbtO2 monitors in severe TBI, discussed extensively throughout this article. She is also an author on several other publications cited throughout the article, most notably BOOST-II and the SIBICC consensus guidelines.
Figures



References
-
- Roozenbeek B, Maas AIR, Menon DK. Changing patterns in the epidemiology of traumatic brain injury. Nat Rev Neurol. 2013. February 26;9(4):231–236. - PubMed
-
- Jourdan C, Bosserelle V, Azerad S, Ghout I, Bayen E, Aegerter P, et al. Predictive factors for 1-year outcome of a cohort of patients with severe traumatic brain injury (TBI): results from the PariS-TBI study. Brain Inj. 2013. June 3;27(9):1000–1007. - PubMed
-
- Cooper DJ, Rosenfeld JV, Murray L, Arabi YM, Davies AR, D’Urso P, et al. Decompressive craniectomy in diffuse traumatic brain injury. N Engl J Med. 2011. April 21;364(16):1493–1502. - PubMed
-
- Steyerberg EW, Wiegers E, Sewalt C, Buki A, Citerio G, De Keyser V, et al. Case-mix, care pathways, and outcomes in patients with traumatic brain injury in CENTER-TBI: a European prospective, multicentre, longitudinal, cohort study. Lancet Neurol. 2019;18(10):923–934. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
