

COVID-19 Imaging: What We Know Now and What Remains Unknown
- PMID: 33560192
- PMCID: PMC7879709
- DOI: 10.1148/radiol.2021204522
COVID-19 Imaging: What We Know Now and What Remains Unknown
Abstract
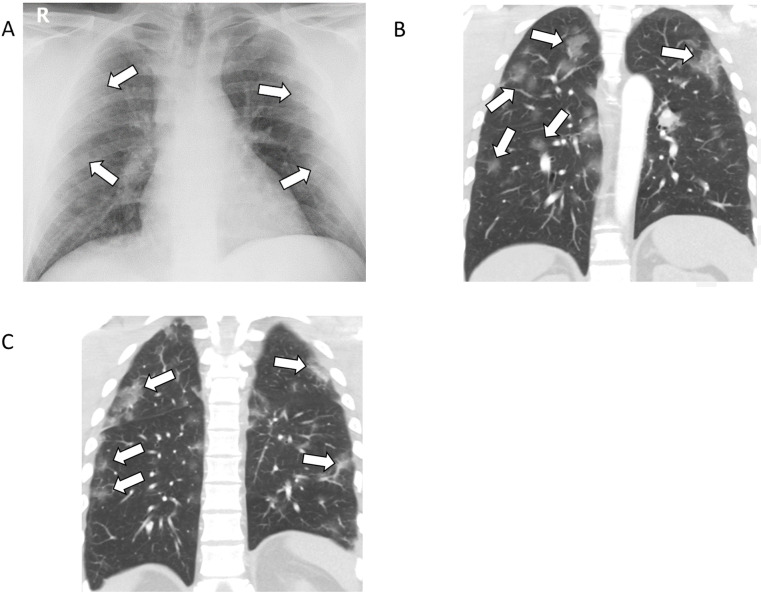
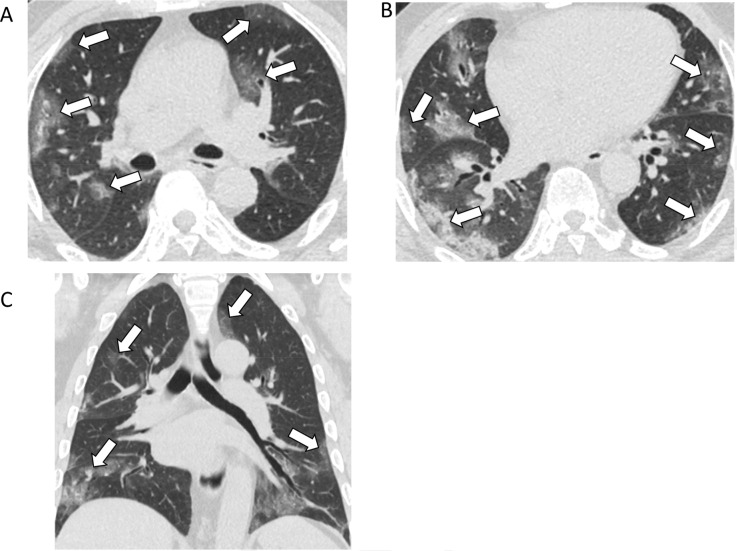
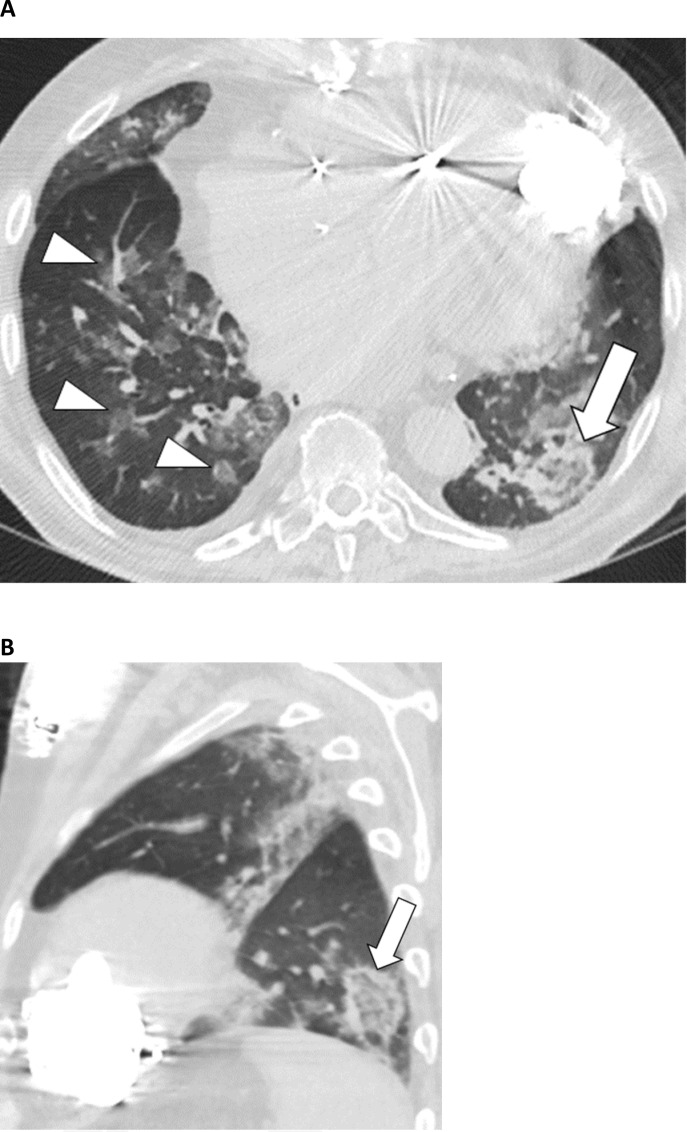
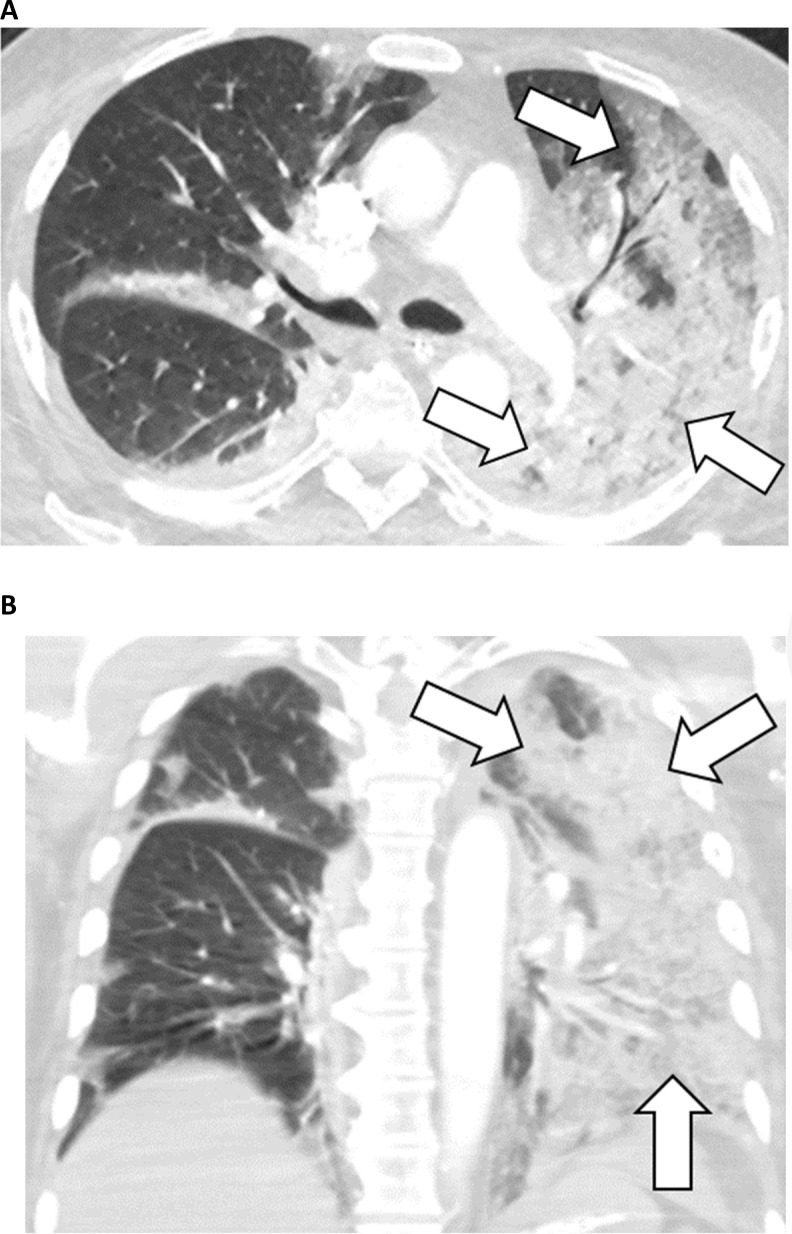
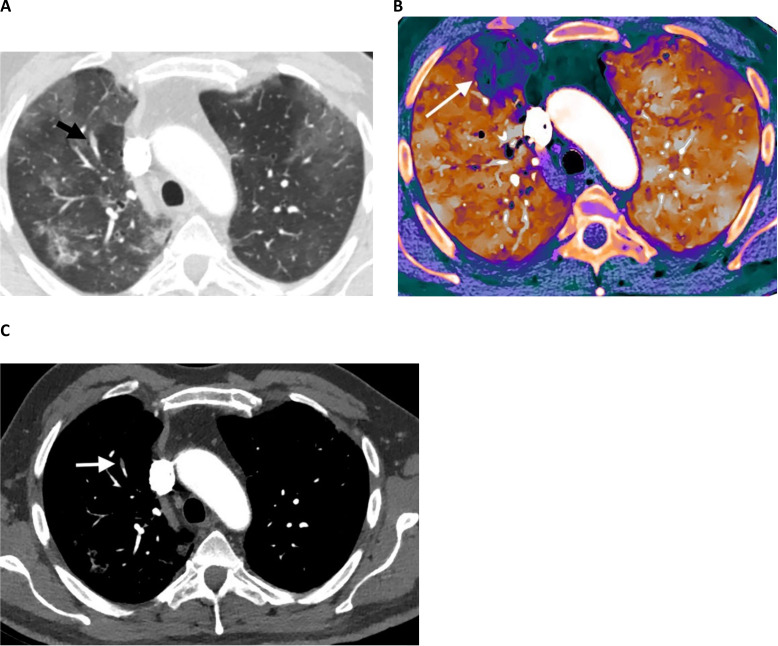
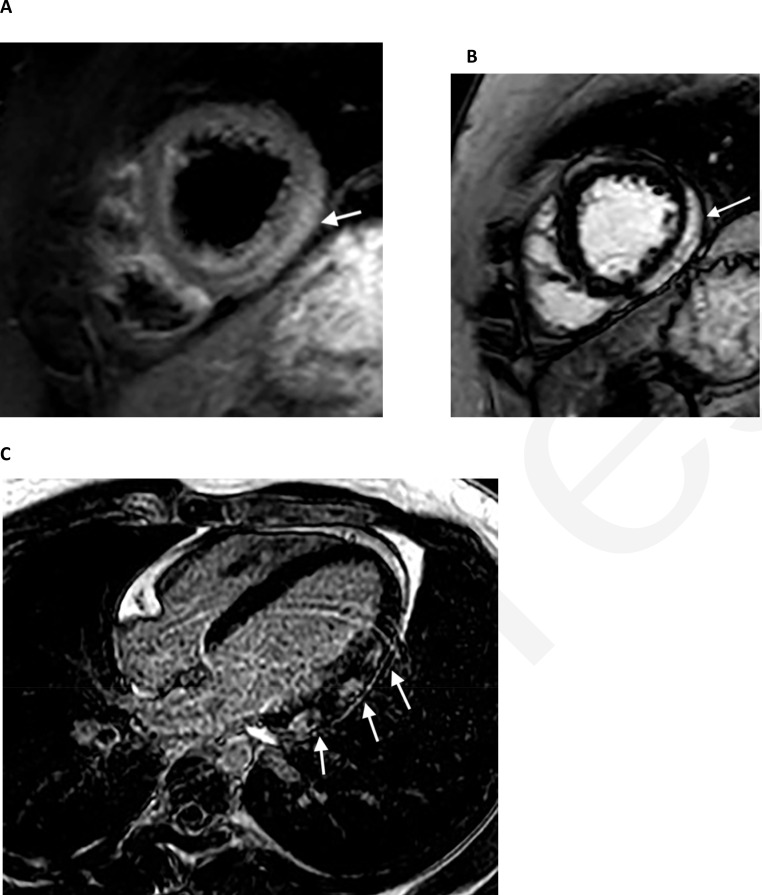
Infection with SARS-CoV-2 ranges from an asymptomatic condition to a severe and sometimes fatal disease, with mortality most frequently being the result of acute lung injury. The role of imaging has evolved during the pandemic, with CT initially being an alternative and possibly superior testing method compared with reverse transcriptase-polymerase chain reaction (RT-PCR) testing and evolving to having a more limited role based on specific indications. Several classification and reporting schemes were developed for chest imaging early during the pandemic for patients suspected of having COVID-19 to aid in triage when the availability of RT-PCR testing was limited and its level of performance was unclear. Interobserver agreement for categories with findings typical of COVID-19 and those suggesting an alternative diagnosis is high across multiple studies. Furthermore, some studies looking at the extent of lung involvement on chest radiographs and CT images showed correlations with critical illness and a need for mechanical ventilation. In addition to pulmonary manifestations, cardiovascular complications such as thromboembolism and myocarditis have been ascribed to COVID-19, sometimes contributing to neurologic and abdominal manifestations. Finally, artificial intelligence has shown promise for use in determining both the diagnosis and prognosis of COVID-19 pneumonia with respect to both radiography and CT.
Figures


Comment in
-
The Cochrane Systematic Review on Thoracic Imaging Tests for the Diagnosis of COVID-19.Radiology. 2021 Jun;299(3):E289. doi: 10.1148/radiol.2021210564. Epub 2021 Mar 23. Radiology. 2021. PMID: 33754831 Free PMC article. No abstract available.
References
-
- American College of Radiology . ACR recommendations for the use of chest radiography and computed tomography (CT) for suspected COVID-19 infection Reston, VA2020. Available from: https://www.acr.org/Advocacy-and-Economics/ACR-Position-Statements/Recom....
-
- Society of Thoracic Radiology . STR/ASER COVID-19 position statement. Society of Thoracic Radiology and American Society of Emergency Radiology, March 11, 2020 2020. Available from: https://thoracicrad.org/?page_id=2879.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
