

Clinical screening tools for obstructive sleep apnea in a population with atrial fibrillation: a diagnostic accuracy trial
- PMID: 33560210
- PMCID: PMC8320498
- DOI: 10.5664/jcsm.9098
Clinical screening tools for obstructive sleep apnea in a population with atrial fibrillation: a diagnostic accuracy trial
Abstract
Study objectives: Although obstructive sleep apnea (OSA) is a known risk factor for atrial fibrillation (AF), there is a paucity of data around its diagnosis and management in patients with AF. The objectives of this study were to compare the diagnostic accuracy of commonly used OSA screening tools in an AF population, including a level 3 portable sleep study device, and to examine the epidemiology of OSA in a hospital cohort with AF.
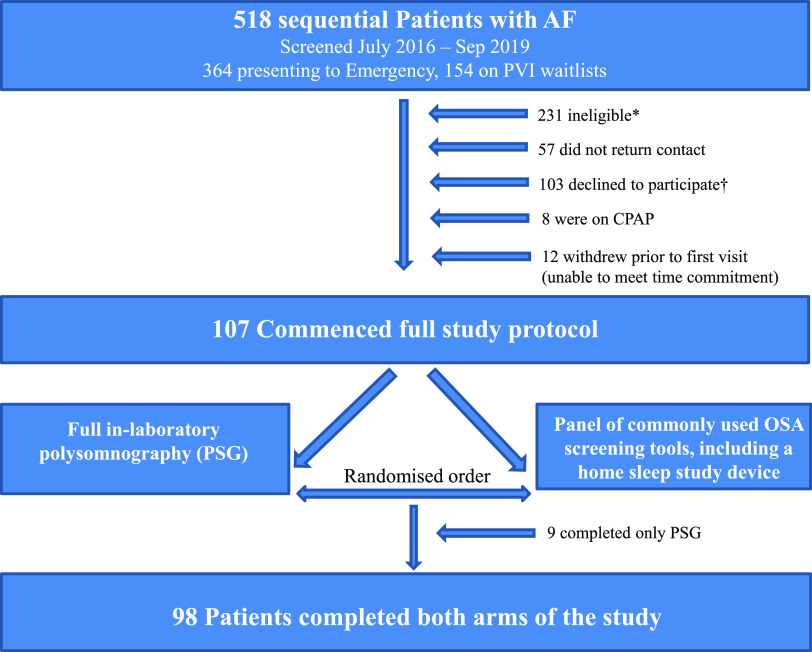
Methods: One hundred seven patients with AF recruited from 2 tertiary centers underwent a panel of OSA screening tools and in-laboratory polysomnography in randomized order.
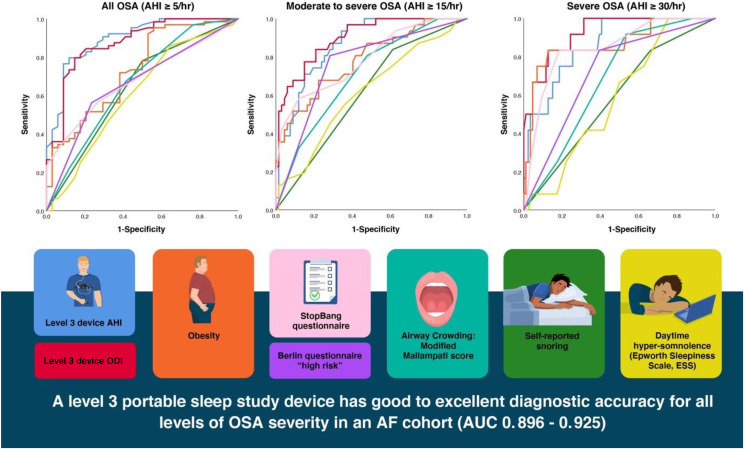
Results: Oxygen desaturation index derived from a level 3 portable sleep study device performed best for moderate to severe and severe OSA, with excellent diagnostic accuracy (area under the curve, 0.899; 95% confidence interval, 0.838-0.960 and area under the curve, 0.925; 95% confidence interval, 0.859-0.991, respectively). Sixty-seven patients (62.6%) were newly diagnosed with OSA (31.8% mild, 18.7% moderate, 12.1% severe).
Conclusions: Undiagnosed OSA is highly prevalent in a hospital AF cohort. However, it is characterized by a relative paucity of symptoms, markedly limiting the usefulness of history or screening questionnaires. This is the first study to find that a level 3 home sleep study device shows excellent diagnostic accuracy in patients with AF. This finding may inform AF management guidelines.
Clinical trial registration: Registry: Australian New Zealand Clinical Trials Registry; Name: The validity and reliability of a portable device for the diagnosis of Obstructive Sleep Apnoea in patients with Atrial Fibrillation; URL:https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=371024; Identifier: ACTRN12616001016426.
Keywords: ApneaLink; apnea-hypopnea index; level 3 sleep study; oxygen desaturation index; polygraphy.
© 2021 American Academy of Sleep Medicine.
Conflict of interest statement
All authors have seen and approved the manuscript. Work for this study was performed at the Royal North Shore Hospital, Sydney, Australia, and the Charles Perkins Centre, University of Sydney, Sydney, Australia. AMM received research grants from the Ramsay Research and Teaching Fund, Sydney, Australia, and the ResMed Foundation/Sleep Health Foundation Research Entry Scholarship administered through the Royal Australasian College of Physicians, Sydney, Australia. AMM reports that in-kind support for this study (loan of ApneaLink Air diagnostic study devices) was received from Resmed Pty Ltd, Sydney, Australia. Resmed played no role in the design or implementation of the study. PAC has an appointment to an endowed academic chair at the University of Sydney that was created from ResMed funding; he receives no personal fees, and this relationship is managed by an oversight committee of the university. PAC has received research support from ResMed, SomnoMed, Zephyr Sleep Technologies, and Bayer; is a consultant/adviser to Zephyr Sleep Technologies, ResMed, SomnoMed, and Signifier Medical Technologies; and has a pecuniary interest in SomnoMed related to a previous role in research and development. KS reports in-kind support from SomnoMed in donation of oral appliances for a previous investigator-initiated research study. The remaining authors report no conflicts of interest.
Figures
Comment in
-
Obstructive sleep apnea and atrial fibrillation: we need to go step by step.J Clin Sleep Med. 2021 May 1;17(5):869-870. doi: 10.5664/jcsm.9242. J Clin Sleep Med. 2021. PMID: 33709908 Free PMC article.
-
Apnea-hypopnea index vs oxygen desaturation index for diagnosis of obstructive sleep apnea in patients with atrial fibrillation: six of one, half a dozen of the other?J Clin Sleep Med. 2021 Nov 1;17(11):2333-2334. doi: 10.5664/jcsm.9524. Epub 2021 Jul 26. J Clin Sleep Med. 2021. PMID: 34666886 Free PMC article. No abstract available.
-
Moving beyond the AHI.J Clin Sleep Med. 2021 Nov 1;17(11):2335-2336. doi: 10.5664/jcsm.9560. Epub 2021 Jul 27. J Clin Sleep Med. 2021. PMID: 34666887 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
