

Prevalence of Bicuspid Aortic Valve and Associated Aortopathy in Newborns in Copenhagen, Denmark
- PMID: 33560321
- PMCID: PMC7873775
- DOI: 10.1001/jama.2020.27205
Prevalence of Bicuspid Aortic Valve and Associated Aortopathy in Newborns in Copenhagen, Denmark
Abstract
Importance: The prevalence and characteristics of bicuspid aortic valve (BAV) are mainly reported from selected cohorts. BAV is associated with aortopathy, but it is unclear if it represents a fetal developmental defect or is secondary to abnormal valve dynamics.
Objective: To determine the prevalence of BAV and BAV subtypes and to describe the associated aortopathy in a large, population-based cohort of newborns.
Design, setting, and participants: The Copenhagen Baby Heart Study was a cross-sectional, population-based study open to all newborns born in Copenhagen between April 1, 2016, and October 31, 2018. Newborns with BAV were matched 1:2 to newborns with a tricuspid aortic valve (non-BAV group) on sex, singleton/twin pregnancy, gestational age, weight, and age at time of examination.
Exposures: Transthoracic echocardiography within 60 days after birth.
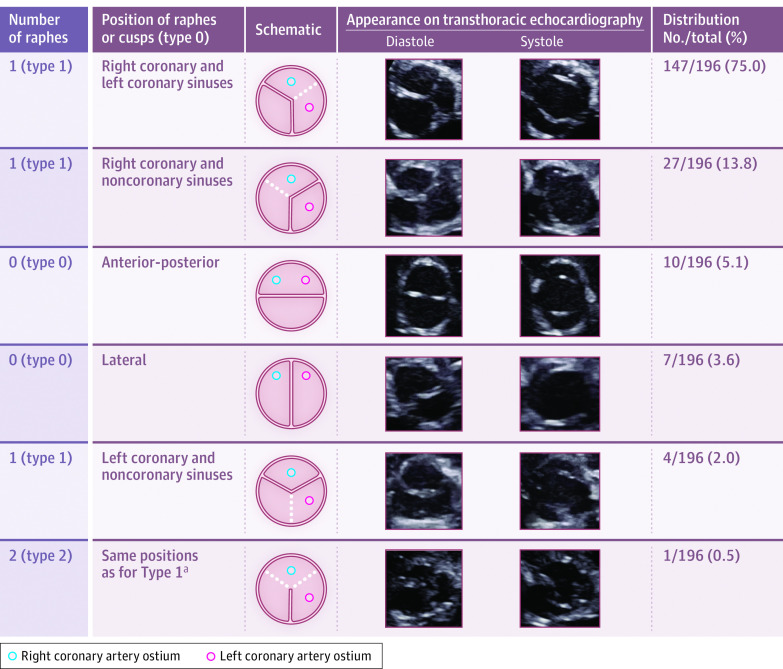
Main outcomes and measures: Primary outcome was BAV prevalence and types, ie, number of raphes and spatial orientation of raphes or cusps (no raphes), according to the classification system of Sievers and Schmidtke (classified as type 0, 1, or 2, with numbers indicating the number of raphes). Secondary outcome was valve function and BAV-associated aortopathy, defined as aortic diameter z score of 3 or greater or coarctation.
Results: In total, 25 556 newborns (51.7% male; mean age, 12 [SD, 8] days) underwent echocardiography. BAV was diagnosed in 196 newborns (prevalence, 0.77% [95% CI, 0.67%-0.88%]), with male-female ratio 2.1:1. BAV was classified as type 0 in 17 newborns (8.7% [95% CI, 5.5%-13.5%]), type 1 in 178 (90.8% [95% CI, 86.0%-94.1%]) (147 [75.0% {95% CI, 68.5%-80.5%}] right-left coronary raphe, 27 [13.8% {95% CI, 9.6%-19.3%}] right coronary-noncoronary raphe, 4 [2.0% {95% CI, 0.8%-5.1%}] left coronary-noncoronary raphe), and type 2 in 1 (0.5% [95% CI, 0.1%-2.8%]). Aortic regurgitation was more prevalent in newborns with BAV (n = 29 [14.7%]) than in those without BAV (1.3%) (absolute % difference, 13.4% [95% CI, 7.8%-18.9%]; P < .001). Newborns with BAV had higher flow velocities across the valve (0.67 [95% CI, 0.65-0.69] m/s vs 0.61 [95% CI, 0.60-0.62] m/s; mean difference, 0.06 m/s [95% CI, 0-0.1]) and larger aortic root and tubular ascending aortic diameters than those without BAV (10.7 [95% CI, 10.7-10.9] mm vs 10.3 [95% CI, 10.2-10.4] mm; mean difference, 0.43 mm [95% CI, 0.2-0.6 mm] and 9.8 [95% CI, 9.6-10.0] mm vs 9.4 [95% CI, 9.3-9.5] mm; mean difference, 0.46 mm [95% CI, 0.30-0.70], respectively) (P < .001 for all). Aortopathy was seen in 65 newborns (33.2%) with BAV (62 with aortic z score ≥3; 3 with coarctation).
Conclusions and relevance: Among newborns in Copenhagen, the prevalence of BAV was 0.77%. Aortopathy was common in newborns with BAV, suggesting that it also represents a fetal malformation.
Conflict of interest statement
Figures
Comment in
-
Bicuspid Aortic Valve-A Common Form of Structural Heart Disease.JAMA. 2021 Feb 9;325(6):540-541. doi: 10.1001/jama.2021.0109. JAMA. 2021. PMID: 33560308 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
