

Diagnosis and Treatment of Hip and Knee Osteoarthritis: A Review
- PMID: 33560326
- PMCID: PMC8225295
- DOI: 10.1001/jama.2020.22171
Diagnosis and Treatment of Hip and Knee Osteoarthritis: A Review
Abstract
Importance: Osteoarthritis (OA) is the most common joint disease, affecting an estimated more than 240 million people worldwide, including an estimated more than 32 million in the US. Osteoarthritis is the most frequent reason for activity limitation in adults. This Review focuses on hip and knee OA.
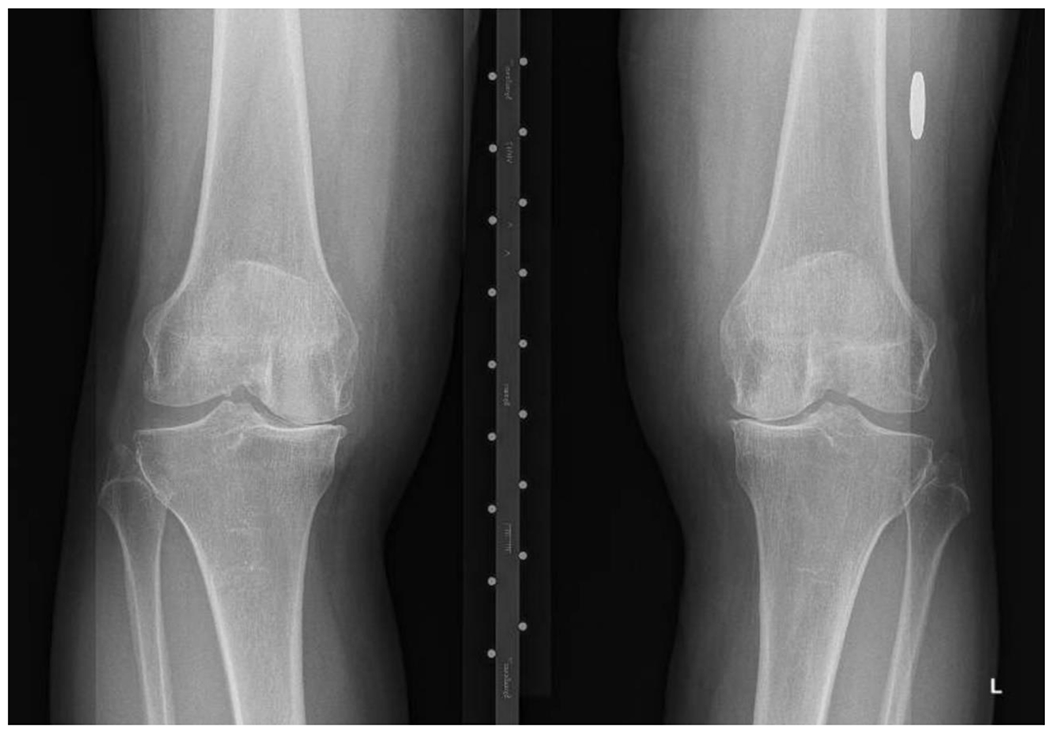
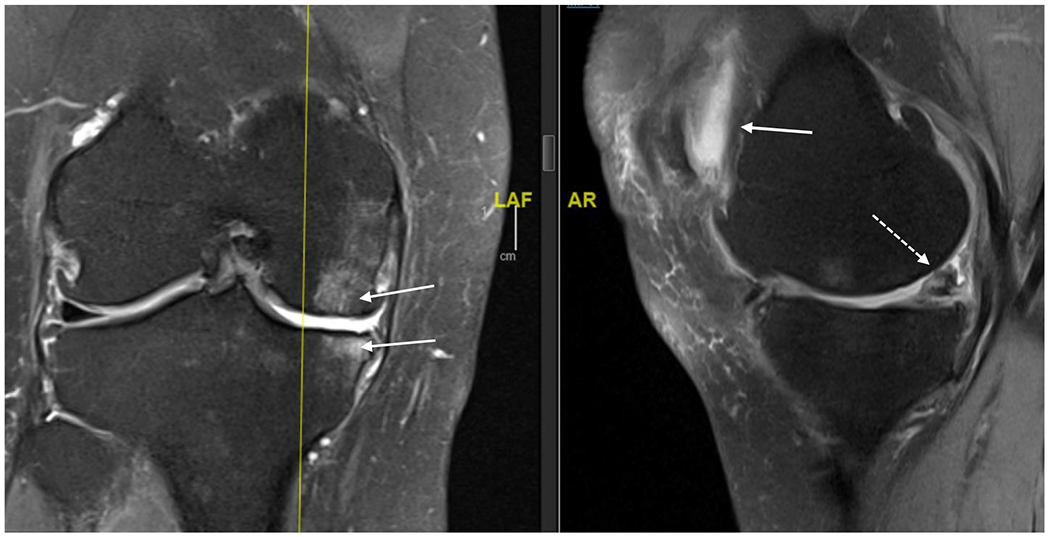
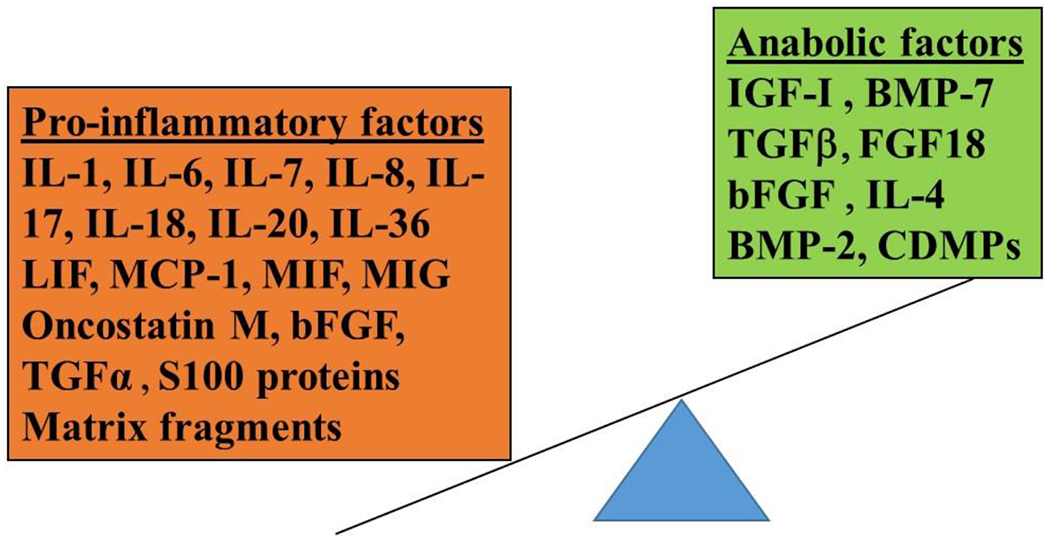
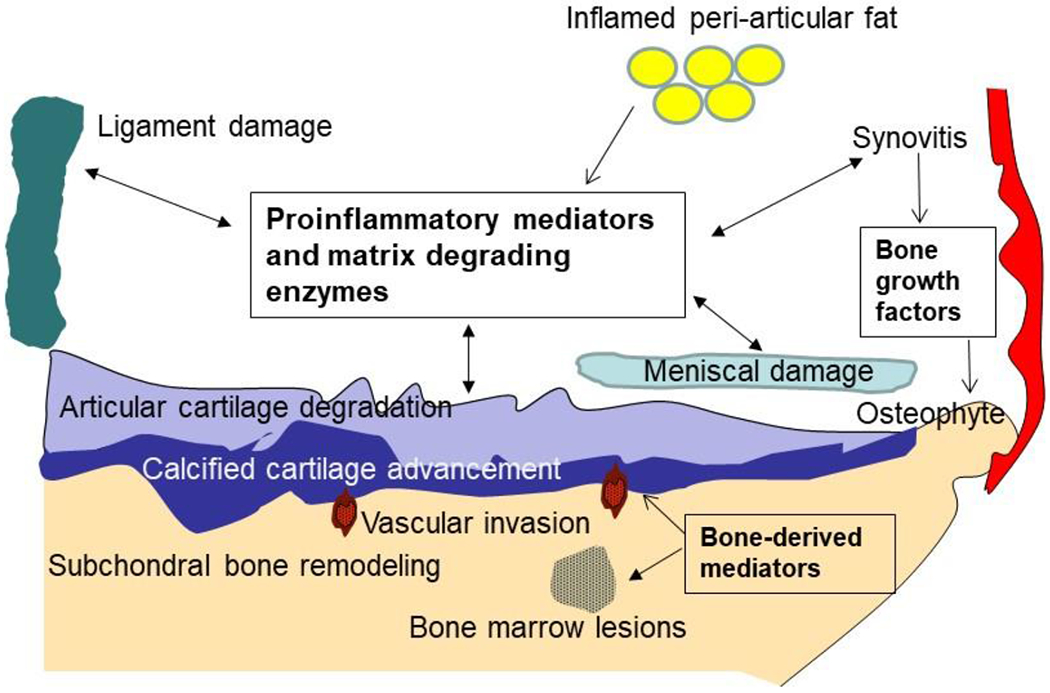
Observations: Osteoarthritis can involve almost any joint but typically affects the hands, knees, hips, and feet. It is characterized by pathologic changes in cartilage, bone, synovium, ligament, muscle, and periarticular fat, leading to joint dysfunction, pain, stiffness, functional limitation, and loss of valued activities, such as walking for exercise and dancing. Risk factors include age (33% of individuals older than 75 years have symptomatic and radiographic knee OA), female sex, obesity, genetics, and major joint injury. Persons with OA have more comorbidities and are more sedentary than those without OA. The reduced physical activity leads to a 20% higher age-adjusted mortality. Several physical examination findings are useful diagnostically, including bony enlargement in knee OA and pain elicited with internal hip rotation in hip OA. Radiographic indicators include marginal osteophytes and joint space narrowing. The cornerstones of OA management include exercises, weight loss if appropriate, and education-complemented by topical or oral nonsteroidal anti-inflammatory drugs (NSAIDs) in those without contraindications. Intra-articular steroid injections provide short-term pain relief and duloxetine has demonstrated efficacy. Opiates should be avoided. Clinical trials have shown promising results for compounds that arrest structural progression (eg, cathepsin K inhibitors, Wnt inhibitors, anabolic growth factors) or reduce OA pain (eg, nerve growth factor inhibitors). Persons with advanced symptoms and structural damage are candidates for total joint replacement. Racial and ethnic disparities persist in the use and outcomes of joint replacement.
Conclusions and relevance: Hip and knee OA are highly prevalent and disabling. Education, exercise and weight loss are cornerstones of management, complemented by NSAIDs (for patients who are candidates), corticosteroid injections, and several adjunctive medications. For persons with advanced symptoms and structural damage, total joint replacement effectively relieves pain.
Figures
Comment in
-
Review of Hip and Knee Osteoarthritis.JAMA. 2021 Jun 22;325(24):2504-2505. doi: 10.1001/jama.2021.6018. JAMA. 2021. PMID: 34156415 No abstract available.
References
-
- Hawker G Osteoarthritis: a serious disease Osteoarthris Research Society International 2016. https://www.oarsi.org/research/oa-serious-disease.
-
- Felson DT, Naimark A, Anderson J, Kazis L, Castelli W, Meenan RF. The prevalence of knee osteoarthritis in the elderly. The Framingham Osteoarthritis Study. Arthritis Rheum. 1987;30(8):914–918. - PubMed
-
- Jordan JM, Helmick CG, Renner JB, et al. Prevalence of knee symptoms and radiographic and symptomatic knee osteoarthritis in African Americans and Caucasians: the Johnston County Osteoarthritis Project. The Journal of Rheumatology. 2007;34(1):172. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
