

Chest pain mimicking pulmonary embolism may be a common presentation of COVID-19 in ambulant patients without other typical features of infection
- PMID: 33560545
- PMCID: PMC8013761
- DOI: 10.1111/joim.13267
Chest pain mimicking pulmonary embolism may be a common presentation of COVID-19 in ambulant patients without other typical features of infection
Abstract
Background: Radiological and pathological studies in severe COVID-19 pneumonia (SARS-CoV-2) have demonstrated extensive pulmonary immunovascular thrombosis and infarction. This study investigated whether these focal changes may present with chest pain mimicking pulmonary emoblism (PE) in ambulant patients.
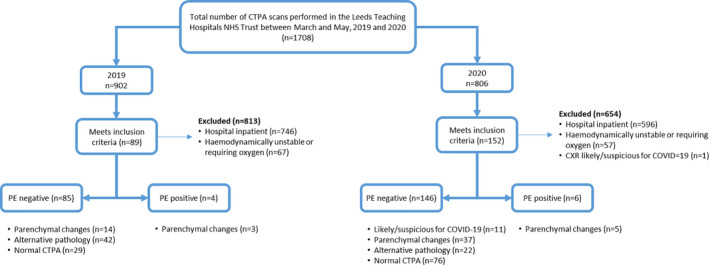
Methods: CTPAs from outpatients presenting with chest pain to Leeds Teaching Hospital NHS Trust 1st March to 31 May 2020 (n = 146) and 2019 (n = 85) were compared. Regions of focal ground glass opacity (GGO), consolidation and/or atelectasis (parenchymal changes) were determined, and all scans were scored using British Society for Thoracic Imaging (BSTI) criteria for COVID-19, and the 2020 cohort was offered SARS-CoV-2 antibody testing.
Results: Baseline demographic and clinical data were similar between groups with absence of fever, normal lymphocytes and marginally elevated CRP and D-Dimer values. Evidence of COVID-19 or parenchymal changes was observed in 32.9% (48/146) of cases in 2020 compared to 16.5% (14/85) in 2019 (P = 0.007). 11/146 (7.5%) patients met BSTI criteria for COVID-19 in 2020 compared with 0/14 in 2019 (P = 0.008). 3/39 patients tested had detectable COVID-19 antibodies (2 with parenchymal changes and 1 with normal parenchyma) however 0/6 patients whose CTPA met BSTI criteria "likely/suspicious for COVID-19" and attended antibody testing were SARS-CoV-2 antibody positive.
Conclusions: 32.8% ambulatory patients with suspected PE in 2020 had parenchymal changes with 7.5% diagnosed as COVID-19 infection by imaging criteria, despite the absence of other COVID-19 symptoms. These findings suggest that localized COVID-19 pneumonitis with immunothrombosis occurs distal to the bronchiolar arteriolar circulation, causing pleural irritation and chest pain without viraemia, accounting for the lack of fever and systemic symptoms.
Keywords: infectious disease; noncardiac chest pain; radiology; thromboembolism.
© 2021 The Authors. Journal of Internal Medicine published by John Wiley & Sons Ltd on behalf of Association for Publication of The Journal of Internal Medicine.
Conflict of interest statement
HMO and DMG are supported by the National Institute for Health Research (NIHR) Leeds Biomedical Research Centre. AS receives salary support from Leeds Cares (Leeds Teaching Hospitals Charitable Foundation) and Innovate UK. The views expressed are those of the authors and not necessarily those of the (UK) National Health Service (NHS), the NIHR or the (UK) Department of Health.
Figures

References
-
- John Hopkins . COVID‐19 Dashboard. [cited 2020 Sep 22]. Available from: https://coronavirus.jhu.edu/map.html
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
