

Impella versus extracorporal life support in cardiogenic shock: a propensity score adjusted analysis
- PMID: 33560591
- PMCID: PMC8006691
- DOI: 10.1002/ehf2.13200
Impella versus extracorporal life support in cardiogenic shock: a propensity score adjusted analysis
Abstract
Aims: The mortality in cardiogenic shock (CS) is high. The role of specific mechanical circulatory support (MCS) systems is unclear. We aimed to compare patients receiving Impella versus ECLS (extracorporal life support) with regard to baseline characteristics, feasibility, and outcomes in CS.
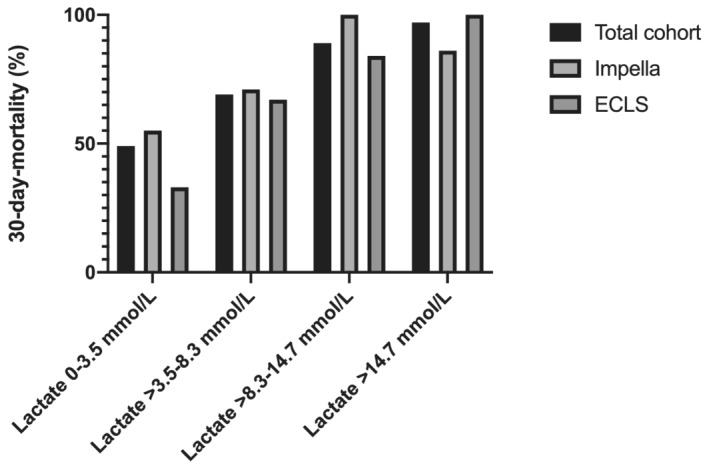
Methods and results: This is a retrospective cohort study including CS patients over 18 years with a complete follow-up of the primary endpoint and available baseline lactate level, receiving haemodynamic support either by Impella 2.5 or ECLS from two European registries. The decision for device implementation was made at the discretion of the treating physician. The primary endpoint of this study was all-cause mortality at 30 days. A propensity score for the use of Impella was calculated, and multivariable logistic regression was used to obtain adjusted odds ratios (aOR). In total, 149 patients were included, receiving either Impella (n = 73) or ECLS (n = 76) for CS. The feasibility of device implantation was high (87%) and similar (aOR: 3.14; 95% CI: 0.18-56.50; P = 0.41) with both systems. The rates of vascular injuries (aOR: 0.95; 95% CI: 0.10-3.50; P = 0.56) and bleedings requiring transfusions (aOR: 0.44; 95% CI: 0.09-2.10; P = 0.29) were similar in ECLS patients and Impella patients. The use of Impella or ECLS was not associated with increased odds of mortality (aOR: 4.19; 95% CI: 0.53-33.25; P = 0.17), after correction for propensity score and baseline lactate level. Baseline lactate level was independently associated with increased odds of 30 day mortality (per mmol/L increase; OR: 1.29; 95% CI: 1.14-1.45; P < 0.001).
Conclusions: In CS patients, the adjusted mortality rates of both ECLS and Impella were high and similar. The baseline lactate level was a potent predictor of mortality and could play a role in patient selection for therapy in future studies. In patients with profound CS, the type of device is likely to be less important compared with other parameters including non-cardiac and neurological factors.
Keywords: Cardiogenic shock; ECMO; Extracorporeal life support; Impella; Mechanical circulatory support.
© 2021 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
The authors have nothing to declare.
Figures
References
-
- Mebazaa A, Combes A, van Diepen S, Hollinger A, Katz JN, Landoni G, Hajjar LA, Lassus J, Lebreton G, Montalescot G, Park JJ. Management of cardiogenic shock complicating myocardial infarction. Intensive Care Med 2018. - PubMed
-
- Feistritzer HJ, Desch S, de Waha S, Jobs A, Zeymer U, Thiele H. German contribution to development and innovations in the management of acute myocardial infarction and cardiogenic shock. Clin Res Cardiol 2018; 107: 74–80. - PubMed
-
- Mebazaa A, Tolppanen H, Mueller C, Lassus J, DiSomma S, Baksyte G, Cecconi M, Choi DJ, Cohen Solal A, Christ M, Masip J, Arrigo M, Nouira S, Ojji D, Peacock F, Richards M, Sato N, Sliwa K, Spinar J, Thiele H, Yilmaz MB, Januzzi J. Acute heart failure and cardiogenic shock: a multidisciplinary practical guidance. Intensive Care Med 2016; 42: 147–163. - PubMed
-
- van Diepen S, Katz JN, Albert NM, Henry TD, Jacobs AK, Kapur NK, Kilic A, Menon V, Ohman EM, Sweitzer NK, Thiele H, Washam JB, Cohen MG, American Heart Association Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; Council on Quality of Care and Outcomes Research; and Mission: Lifeline . Contemporary management of cardiogenic shock: a scientific statement from the American Heart Association. Circulation 2017; 136: e232–e268. - PubMed
-
- Werdan K, Gielen S, Ebelt H, Hochman JS. Mechanical circulatory support in cardiogenic shock. Eur Heart J 2014; 35: 156–167. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
