

Hepatocellular carcinoma in patients coinfected with hepatitis B or C and HIV: more aggressive tumor behavior?
- PMID: 33560682
- PMCID: PMC9446514
- DOI: 10.1097/MEG.0000000000002057
Hepatocellular carcinoma in patients coinfected with hepatitis B or C and HIV: more aggressive tumor behavior?
Abstract
Introduction and objectives: Hepatocellular carcinoma (HCC) is the 6th cause of cancer and hepatitis C (HCV) and B (HBV) viruses are the most frequent risk factors for HCC. Patients coinfected with HCV or HBV and HIV present a faster progression to liver fibrosis and higher incidence of HCC. The aim of this study was to evaluate the survival and clinical outcomes of coinfected patients with HCC comparing with non-HIV patients.
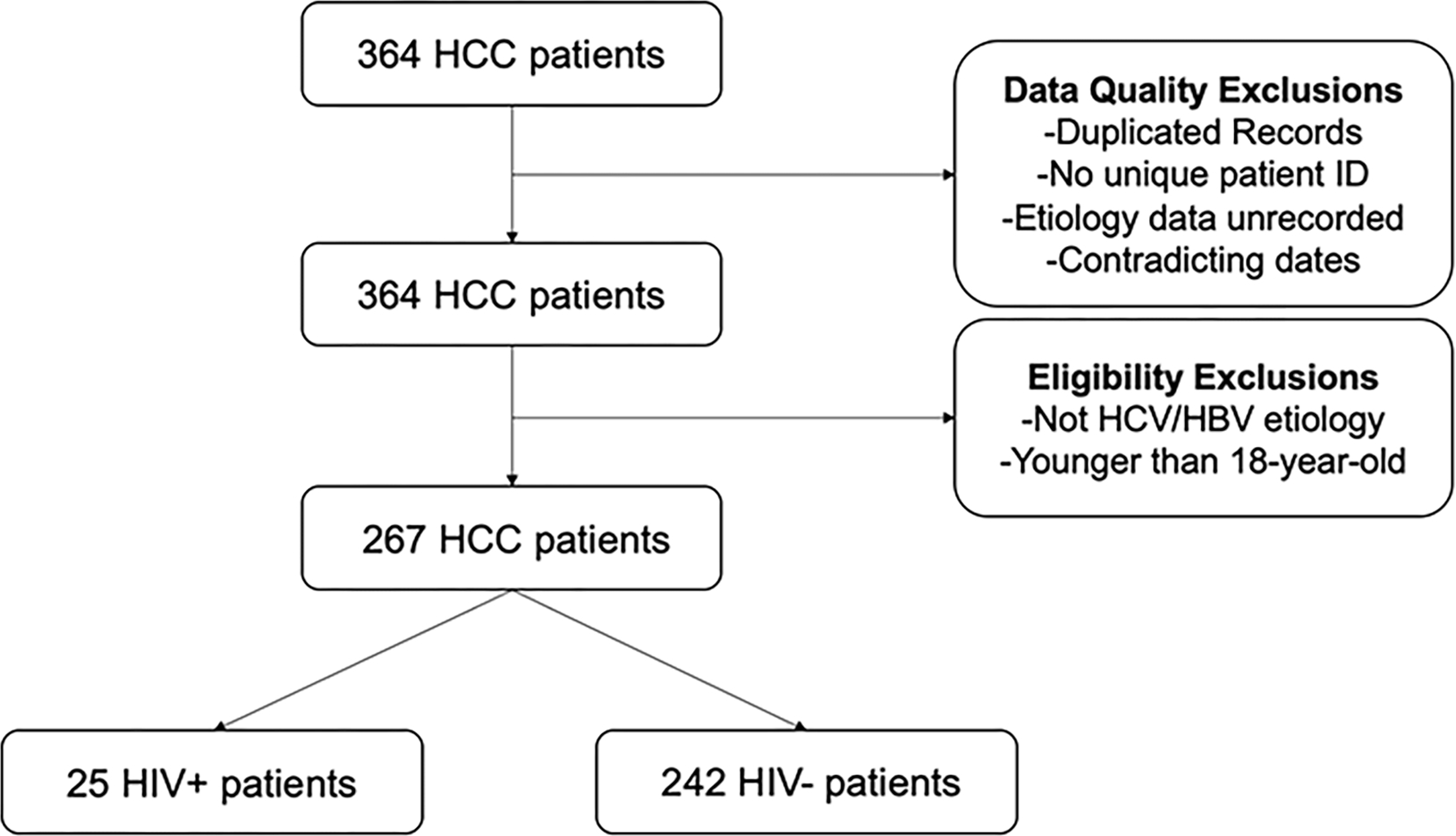
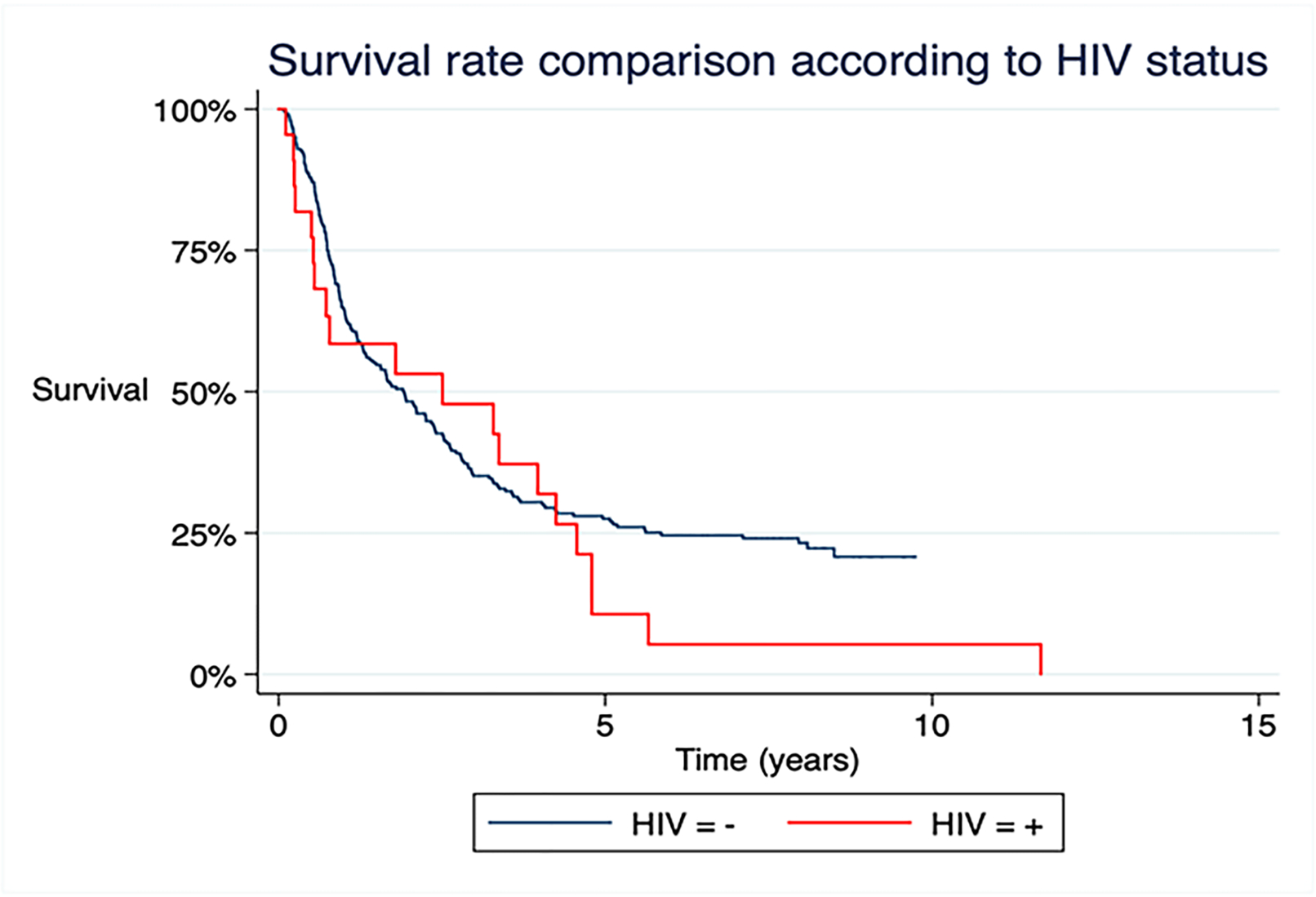
Methods: We conducted a retrospective cohort study, including 267 HCC patients with HCV or HBV infection with or without HIV. The primary endpoint was overall survival. A Kaplan-Meier curve was presented to assess survival function. Clinical and radiologic variables, according to HIV status, were compared by logistic regression.
Results: Among 267 HCC patients, 25 (9.3%) were HIV-positive. In the coinfected group, patients were younger (49.8 vs 61.2 years, P < 0.001), cirrhosis was less predominant (88 vs 96.7%, P = 0.05), a smaller proportion received HCC treatment (60 vs 86.3%, P = 0.001) and the frequency of portal vein tumoral thrombosis was higher (32 vs 11.1%, P = 0.003). The overall mortality rate was higher in the HIV-positive group (92 vs 74.3%), independently of clinical and tumoral variables.
Conclusion: Coinfected patients with HCC presented higher mortality, tumor diagnosis in a younger age, less underlying cirrhosis and a higher frequency of tumoral thrombosis. Further studies are warranted to better understand the role of HIV in hepatocarcinogenesis, in order to improve the management of those patients, particularly regarding screening programs.
Copyright © 2020 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. - PubMed
-
- Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018;391(10127):1301–14. - PubMed
-
- Bruix J, Sherman M. Management of hepatocellular carcinoma. Hepatology. 2005;42(5):1208–36. - PubMed
-
- Pinato DJ, Pria AD, Sharma R, Bower M. Hepatocellular carcinoma: An evolving challenge in viral hepatitis and HIV coinfection. Aids. 2017;31(5):603–11. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
