

Healthcare Patterns of Pregnant Women and Children Affected by OUD in 9 State Medicaid Populations
- PMID: 33560699
- PMCID: PMC8339176
- DOI: 10.1097/ADM.0000000000000780
Healthcare Patterns of Pregnant Women and Children Affected by OUD in 9 State Medicaid Populations
Abstract
Objectives: State Medicaid programs are the largest single provider of healthcare for pregnant persons with opioid use disorder (OUD). Our objective was to provide comparable, multistate measures estimating the burden of OUD in pregnancy, medication for OUD (MOUD) in pregnancy, and related neonatal and child outcomes.
Methods: Drawing on the Medicaid Outcomes Distributed Research Network (MODRN), we accessed administrative healthcare data for 1.6 million pregnancies and 1.3 million live births in 9 state Medicaid populations from 2014 to 2017. We analyzed within- and between-state prevalences and time trends in the following outcomes: diagnosis of OUD in pregnancy, initiation, and continuity of MOUD in pregnancy, Neonatal Opioid Withdrawal Syndrome (NOWS), and well-child visit utilization among children with NOWS.
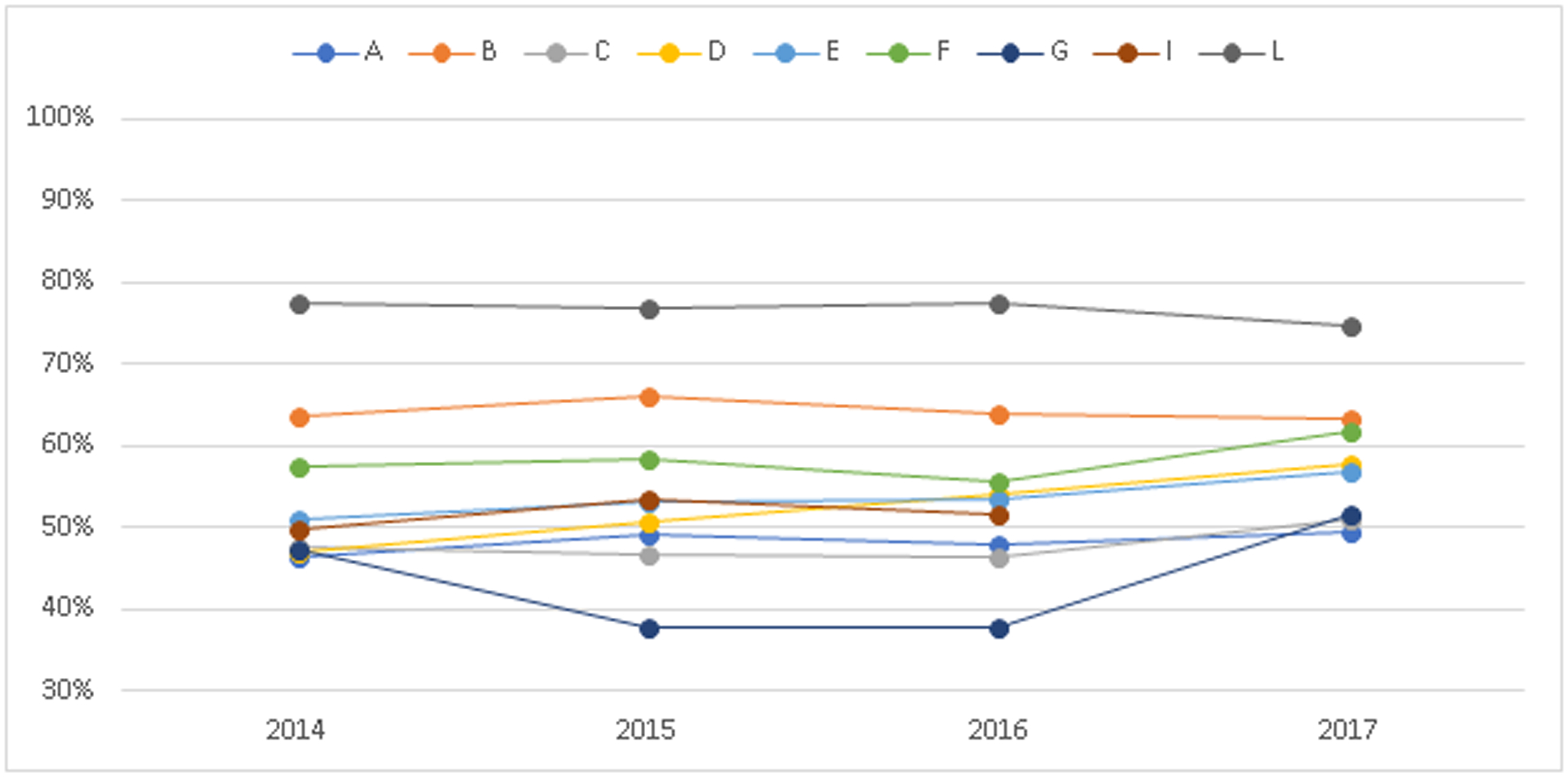
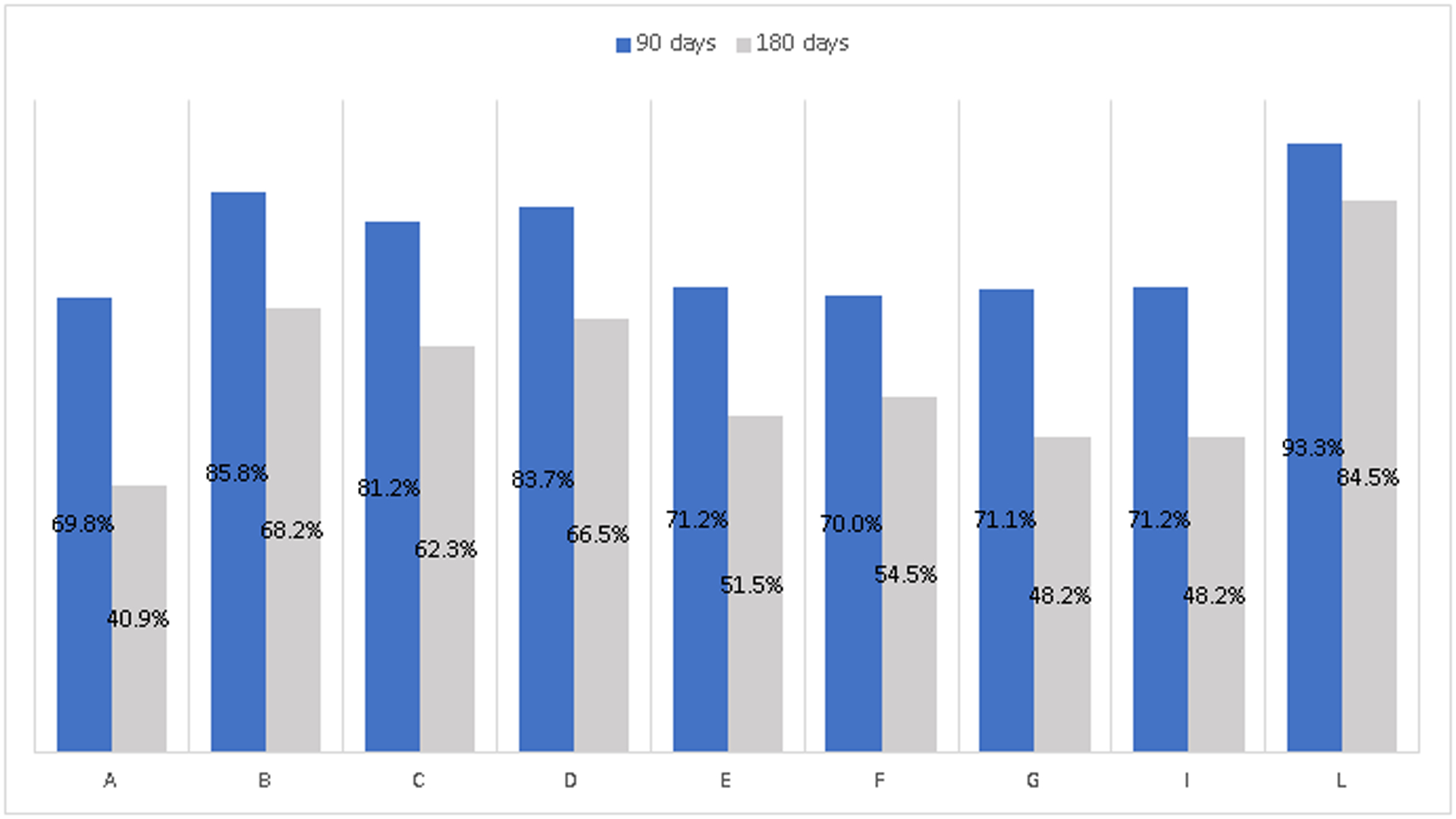
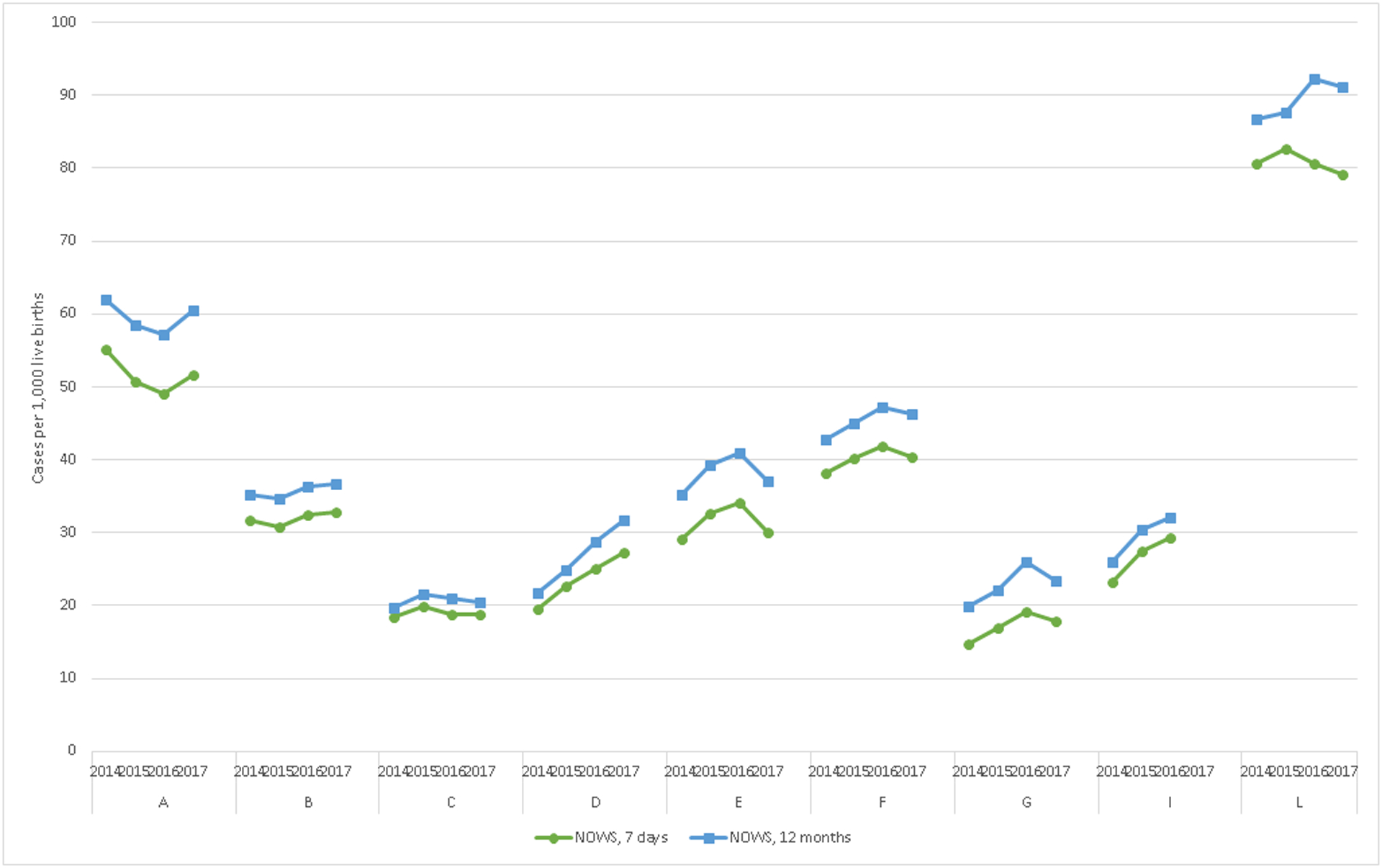
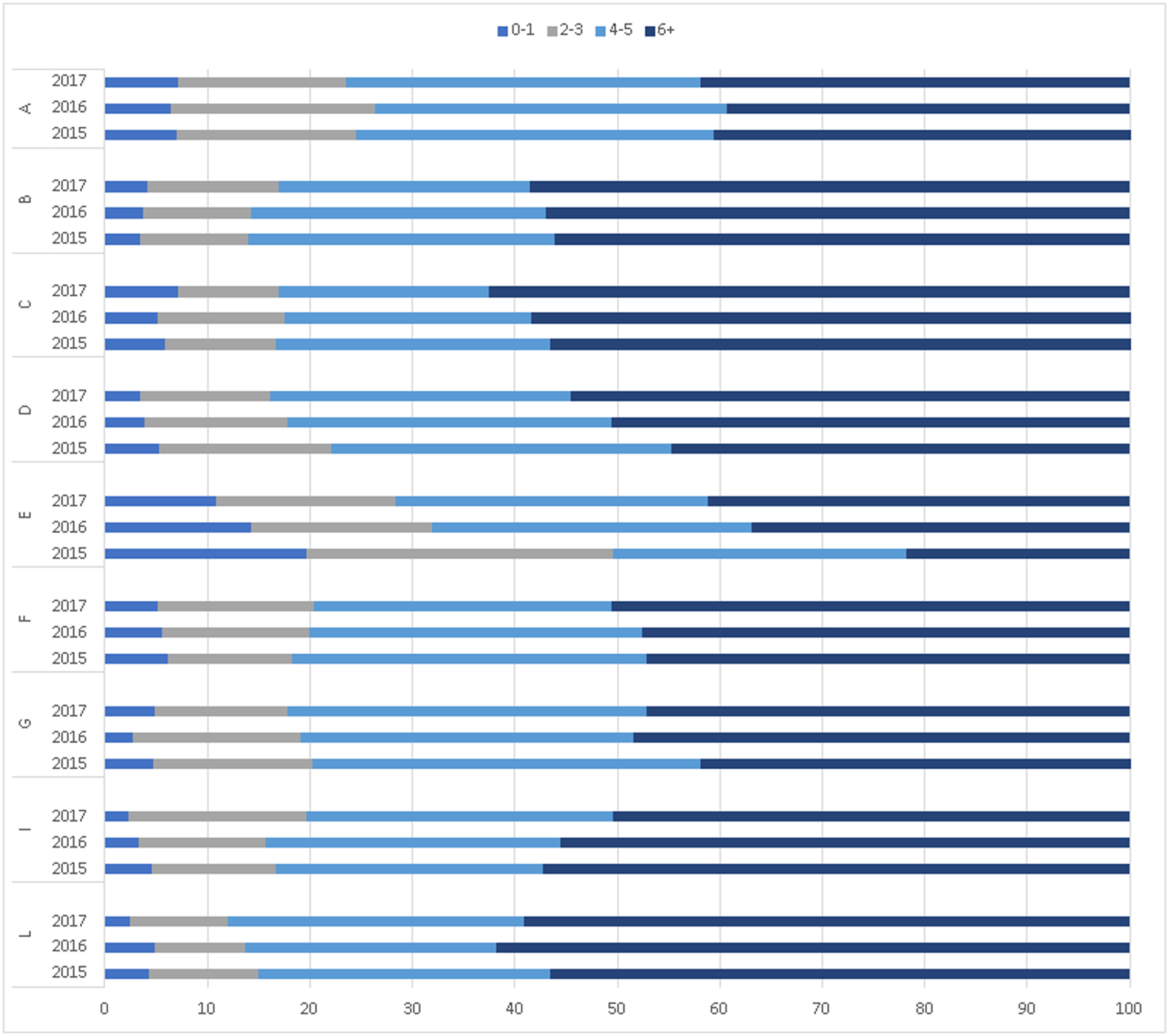
Results: OUD diagnosis increased from 49.6 per 1000 to 54.1 per 1000 pregnancies, and the percentage of those with any MOUD in pregnancy increased from 53.4% to 57.9%, during our study time period. State-specific percentages of 180-day continuity of MOUD ranged from 41.2% to 84.5%. The rate of neonates diagnosed with NOWS increased from 32.7 to 37.0 per 1000 live births. State-specific percentages of children diagnosed with NOWS who had the recommended well-child visits in the first 15 months ranged from 39.3% to 62.5%.
Conclusions: Medicaid data, which allow for longitudinal surveillance of care across different settings, can be used to monitor OUD and related pregnancy and child health outcomes. Findings highlight the need for public health efforts to improve care for pregnant persons and children affected by OUD.
Copyright © 2021 American Society of Addiction Medicine.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Substance Abuse and Mental Health Services Administration. Clinical Guidance for Treating Pregnant and Parenting Women with Opioid Use Disorder and Their Infants. . HHS Publication No. (SMA) 18–5054. Rockville, MD: 2018.
-
- ACOG Committee on Health Care for Underserved Women and American Society of Addiction Medicine. ACOG Committee Opinion No. 524: Opioid abuse, dependence, and addiction in pregnancy. Obstetrics and gynecology. 2012;119(5):1070–1076. - PubMed
-
- Saunders JB, Jarlenski MP, Levy R, Kozhimannil KB. Federal and State Policy Efforts to Address Maternal Opioid Misuse: Gaps and Challenges. Womens Health Issues. 2018;28(2):130–136. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
