

Poor cardiovascular health is associated with subclinical atherosclerosis in apparently healthy sub-Saharan African populations: an H3Africa AWI-Gen study
- PMID: 33563289
- PMCID: PMC7874493
- DOI: 10.1186/s12916-021-01909-6
Poor cardiovascular health is associated with subclinical atherosclerosis in apparently healthy sub-Saharan African populations: an H3Africa AWI-Gen study
Abstract
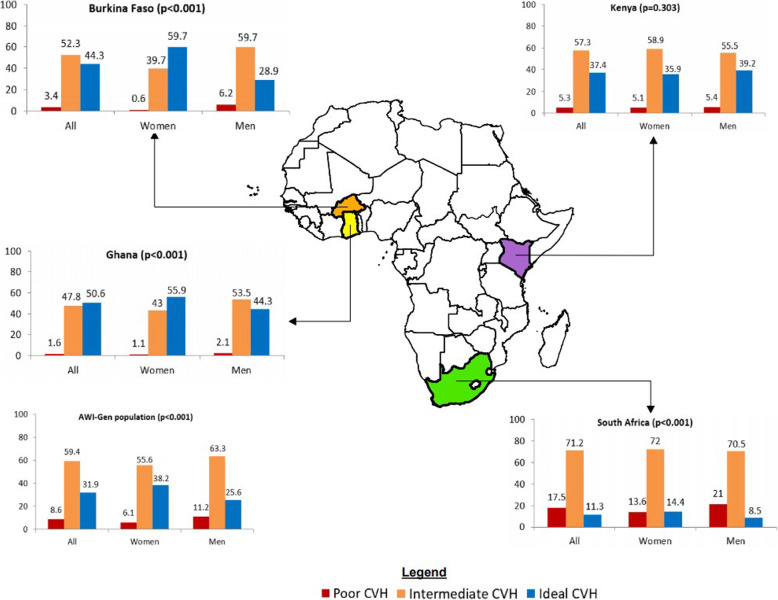
Background: The cardiovascular health index (CVHI) introduced by the American Heart Association is a valid, accessible, simple, and translatable metric for monitoring cardiovascular health in a population. Components of the CVHI include the following seven cardiovascular risk factors (often captured as life's simple 7): smoking, dietary intake, physical activity, body mass index, blood pressure, glucose, and total cholesterol. We sought to expand the evidence for its utility to under-studied populations in sub-Saharan Africa, by determining its association with common carotid intima-media thickness (CIMT).
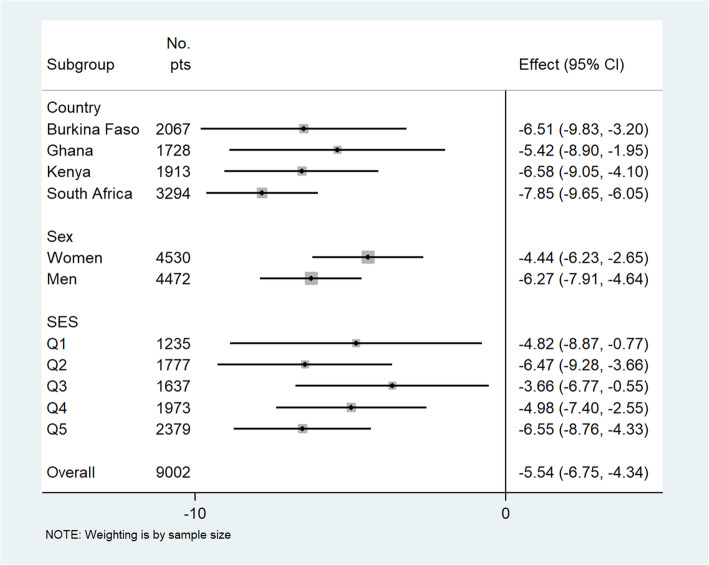
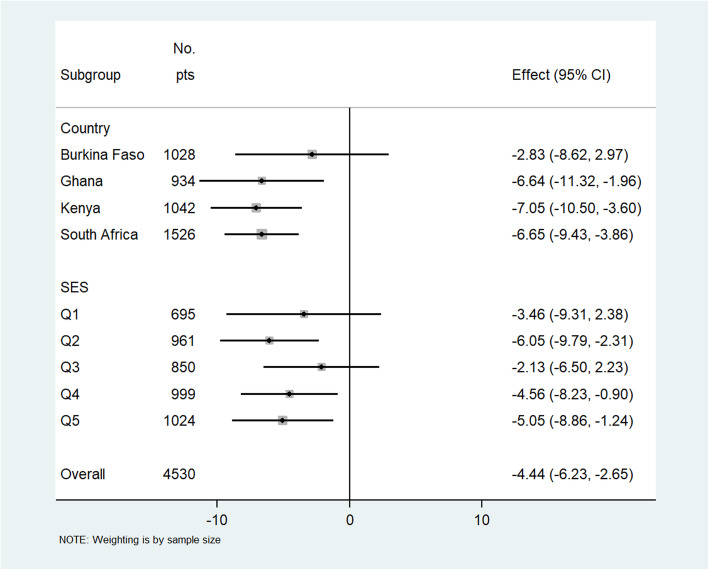
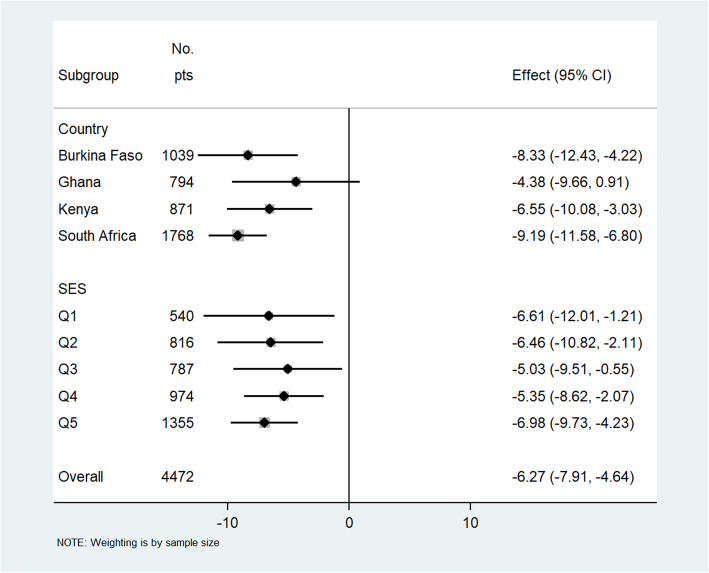
Methods: We conducted a cross-sectional study involving 9011 participants drawn from Burkina Faso, Ghana, Kenya, and South Africa. We assessed established classical cardiovascular risk factors and measured carotid intima-media thickness of the left and right common carotid arteries using B-mode ultrasonography. Adjusted multilevel mixed-effect linear regression was used to determine the association of CVHI with common CIMT. In the combined population, an individual participant data meta-analyses random-effects was used to conduct pooled comparative sub-group analyses for differences between countries, sex, and socio-economic status.
Results: The mean age of the study population was 51 ± 7 years and 51% were women, with a mean common CIMT of 637 ± 117 μm and CVHI score of 10.3 ± 2.0. Inverse associations were found between CVHI and common CIMT (β-coefficients [95% confidence interval]: Burkina Faso, - 6.51 [- 9.83, - 3.20] μm; Ghana, - 5.42 [- 8.90, - 1.95]; Kenya, - 6.58 [- 9.05, - 4.10]; and South Africa, - 7.85 [- 9.65, - 6.05]). Inverse relations were observed for women (- 4.44 [- 6.23, - 2.65]) and men (- 6.27 [- 7.91, - 4.64]) in the pooled sample. Smoking (p < 0.001), physical activity (p < 0.001), and hyperglycemia (p < 0.001) were related to CIMT in women only, while blood pressure and obesity were related to CIMT in both women and men (p < 0.001).
Conclusion: This large pan-African population study demonstrates that CVHI is a strong marker of subclinical atherosclerosis, measured by common CIMT and importantly demonstrates that primary prevention of atherosclerotic cardiovascular disease in this understudied population should target physical activity, smoking, obesity, hypertension, and hyperglycemia.
Keywords: Cardiovascular diseases; Cardiovascular health index; Carotid intima-media thickness; Primary prevention; Screening; Sub-Saharan Africa; Subclinical atherosclerosis; Understudied populations.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- GBD 2015 Risk Factors Collaborators Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1659–1724. doi: 10.1016/S0140-6736(16)31679-8. - DOI - PMC - PubMed
-
- Bawah A, Houle B, Alam N, Razzaque A, Streatfield PK, Debpuur C, et al. The evolving demographic and health transition in four low- and middle-income countries: evidence from four sites in the INDEPTH network of longitudinal health and demographic surveillance systems. Plos One. 2016;11(6):e0157281. doi: 10.1371/journal.pone.0157281. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
