

Extended-Spectrum β-Lactamase and Carbapenemase Producing Gram-Negative Bacilli Infections Among Patients in Intensive Care Units of Felegehiwot Referral Hospital: A Prospective Cross-Sectional Study
- PMID: 33564247
- PMCID: PMC7867495
- DOI: 10.2147/IDR.S292246
Extended-Spectrum β-Lactamase and Carbapenemase Producing Gram-Negative Bacilli Infections Among Patients in Intensive Care Units of Felegehiwot Referral Hospital: A Prospective Cross-Sectional Study
Abstract
Background: Owing to the specific risk profile of its residents, intensive care units (ICUs) are the best place for selection pressure and the epicenter for resistance development and dissemination. Infections with β-lactamase releasing Gram-negative bacilli (GNB) at ICUs are an emerging global threat. This study dogged the magnitude of extended-spectrum β-lactamase (ESBL) and carbapenemase releasing Gram-negative bacilli infections and associated factors among patients in the ICUs of Felegehiwot Referral Hospital, Ethiopia.
Methods: A cross-sectional study was done through February to June 2020. Wound swabs, urine, blood and sputum samples were collected from patients in the ICUs symptomatic for infections while excluding those under coma and shock. Bacterial species were verified using standard microbiological methods. Carbapenemase and ESBL production were identified using modified carbapenem inactivation and combined disk diffusion methods, respectively. Multivariable analysis was calculated for factors associated with ESBL production. P-value < 0.05 was taken as cut-off for statistical significance.
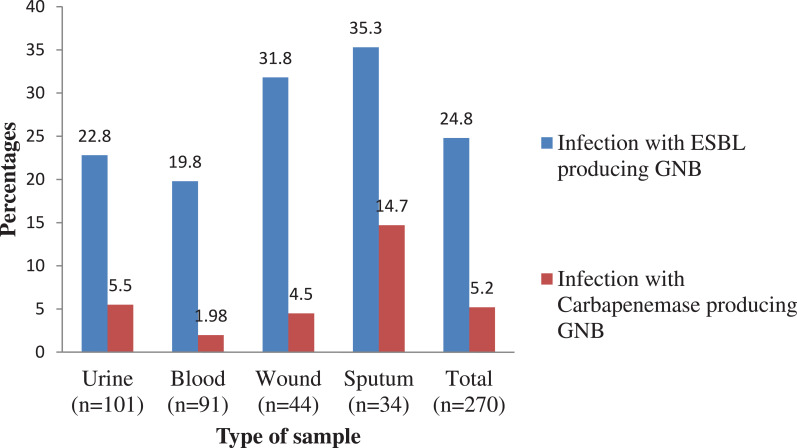
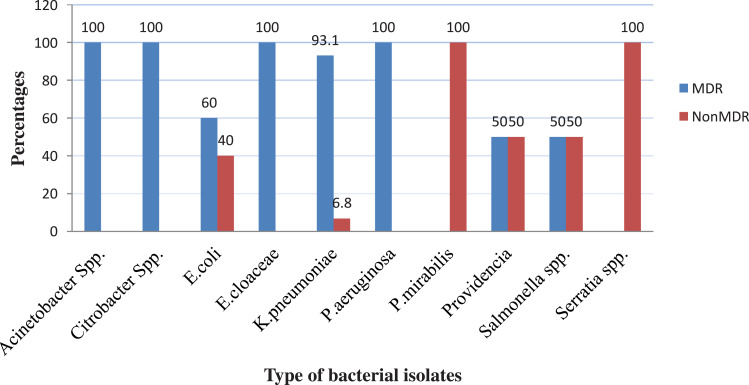
Results: Out of 270 patients in the ICU, 67 (24.8%) and 14 (5.2%) had infections with ESBL and carbapenemase releasing GNB, respectively. The most frequent ESBL producing isolates were P. aeruginosa (100%), E. cloacae (100%), K. pneumoniae (82.8%) and E. coli (64%). The predominant carbapenemase producer isolates were K. pneumoniae (27.6%) and E. cloacae (33.3%). Overall, 77 (81.1%) of species were multi-drug resistant. All GNB species were 100% resistant to tetracycline and ampicillin. They are also resistant to cefuroxime, ceftazidime, sulfamethoxazole-trimethoprim and cefotaxime. Prior hospitalization (AOR = 5.5, CI = 2.63-11.46), support with medical care devices (AOR = 23.7, CI = 4.6-12) and arterial intravenous catheterization (AOR = 2.7, CI = 1.3-5.3) had significant association with β-lactamase producing GNB infection.
Conclusion: Infection with ESBL and carbapenemase producing Gram-negative bacilli linked with an alarming degree of multi-drug resistant isolates is a major healthcare threat among patients in ICUs. Hence, strict adherence to infection prevention practices and wise use of antibiotics are recommended to slow the spread of antimicrobial resistance.
Keywords: ESBL; Ethiopia; FHRH; GNB; ICU; carbapenemase; multi-drug resistance.
© 2021 Alebel et al.
Conflict of interest statement
The authors declared that they have no conflicts of interest for this work.
Figures
Similar articles
-
Multidrug resistance and extended-spectrum beta-lactamase producing Gram-negative bacteria from three Referral Hospitals of Amhara region, Ethiopia.Ann Clin Microbiol Antimicrob. 2021 Mar 11;20(1):16. doi: 10.1186/s12941-021-00422-1. Ann Clin Microbiol Antimicrob. 2021. PMID: 33706775 Free PMC article.
-
High burden of ESBL and carbapenemase-producing gram-negative bacteria in bloodstream infection patients at a tertiary care hospital in Addis Ababa, Ethiopia.PLoS One. 2023 Jun 27;18(6):e0287453. doi: 10.1371/journal.pone.0287453. eCollection 2023. PLoS One. 2023. PMID: 37368908 Free PMC article.
-
High prevalence of fecal carriage of Extended-spectrum beta-lactamase and carbapenemase-producing Enterobacteriaceae among food handlers at the University of Gondar, Northwest Ethiopia.PLoS One. 2022 Mar 17;17(3):e0264818. doi: 10.1371/journal.pone.0264818. eCollection 2022. PLoS One. 2022. PMID: 35298493 Free PMC article.
-
Prevalence of multidrug-resistant and extended-spectrum beta-lactamase (ESBL)-producing gram-negative bacilli: A meta-analysis report in Ethiopia.Drug Target Insights. 2020 Oct 5;14:16-25. doi: 10.33393/dti.2020.2170. eCollection 2020. Drug Target Insights. 2020. PMID: 33132695 Free PMC article. Review.
-
Cefiderocol: A Siderophore Cephalosporin with Activity Against Carbapenem-Resistant and Multidrug-Resistant Gram-Negative Bacilli.Drugs. 2019 Feb;79(3):271-289. doi: 10.1007/s40265-019-1055-2. Drugs. 2019. PMID: 30712199 Review.
Cited by
-
Characteristics of Carbapenem-Resistant Gram-Negative Bacilli in Patients with Ventilator-Associated Pneumonia.Antibiotics (Basel). 2021 Oct 29;10(11):1325. doi: 10.3390/antibiotics10111325. Antibiotics (Basel). 2021. PMID: 34827263 Free PMC article.
-
Antimicrobial resistance profile and associated factors of hospital-acquired gram-negative bacterial pathogens among hospitalized patients in northeast Ethiopia.BMC Microbiol. 2024 Sep 11;24(1):339. doi: 10.1186/s12866-024-03485-0. BMC Microbiol. 2024. PMID: 39261762 Free PMC article.
-
Extended-Spectrum Beta-Lactamase and Carbapenem-Resistant Gram-Negative Pathogens in Makkah, Saudi Arabia.Ethiop J Health Sci. 2022 Nov;32(6):1221-1230. doi: 10.4314/ejhs.v32i6.20. Ethiop J Health Sci. 2022. PMID: 36475249 Free PMC article.
-
Prevalence of carbapenemase-producing Enterobacteriaceae from human clinical samples in Ethiopia: a systematic review and meta-analysis.BMC Infect Dis. 2023 May 3;23(1):277. doi: 10.1186/s12879-023-08237-5. BMC Infect Dis. 2023. PMID: 37138285 Free PMC article.
-
Antimicrobial resistance pattern of Acinetobacter baumannii clinical isolate in Ethiopia. A systematic review and meta-analysis.BMC Infect Dis. 2025 Apr 12;25(1):518. doi: 10.1186/s12879-025-10923-5. BMC Infect Dis. 2025. PMID: 40221655 Free PMC article.
References
-
- Deptuła A, Trejnowska E, Ozorowski T, Hryniewicz W. Risk factors for healthcare-associated infection in light of two years of experience with the ECDC point prevalence survey of healthcare-associated infection and antimicrobial use in Poland. J Hosp Infect. 2015;90(4):310–315. doi:10.1016/j.jhin.2015.03.005 - DOI - PubMed
-
- Khan HA, Baig FK, Mehboob R. Nosocomial infections: epidemiology, prevention, control and surveillance. Asian Pac J Trop Biomed. 2017;7(5):478–482. doi:10.1016/j.apjtb.2017.01.019 - DOI
LinkOut - more resources
Full Text Sources
Other Literature Sources
