

A Simple Protocol to Effectively Manage Anal Fistulas with No Obvious Internal Opening
- PMID: 33564257
- PMCID: PMC7866917
- DOI: 10.2147/CEG.S291909
A Simple Protocol to Effectively Manage Anal Fistulas with No Obvious Internal Opening
Abstract
Purpose: In some anal fistulas, the internal/primary opening cannot be located even after examination and assessment on MRI or transrectal ultrasound. The efficacy of a simple new protocol to manage such therapeutically challenging fistulas was tested.
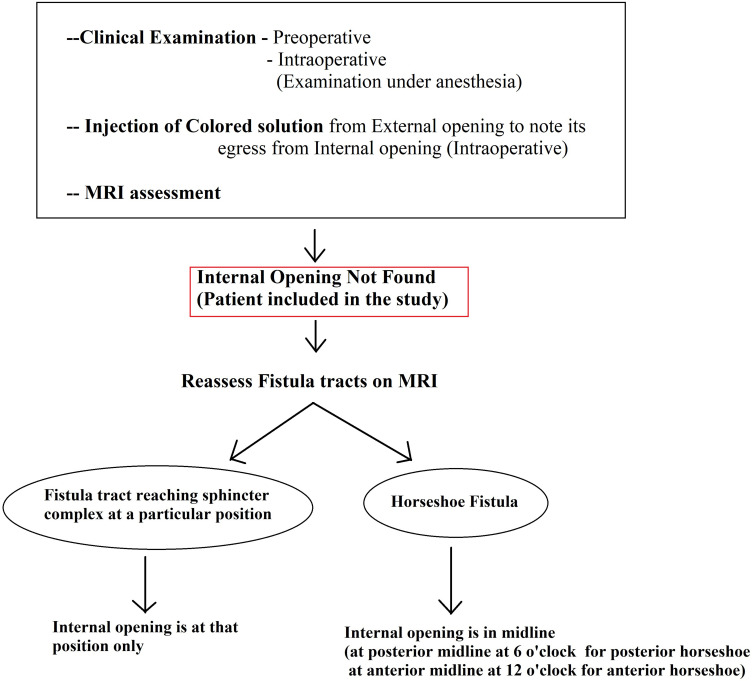
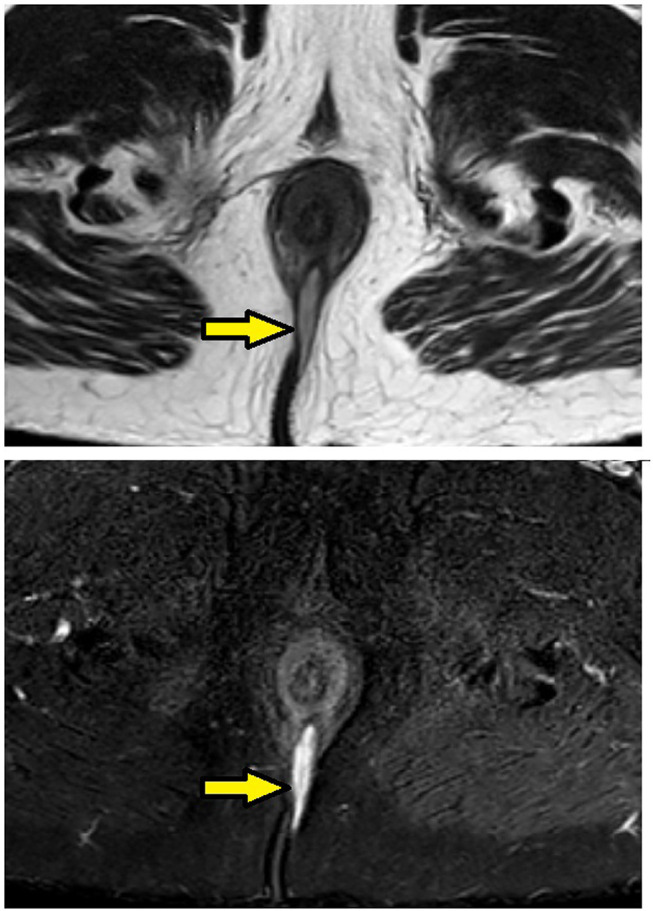
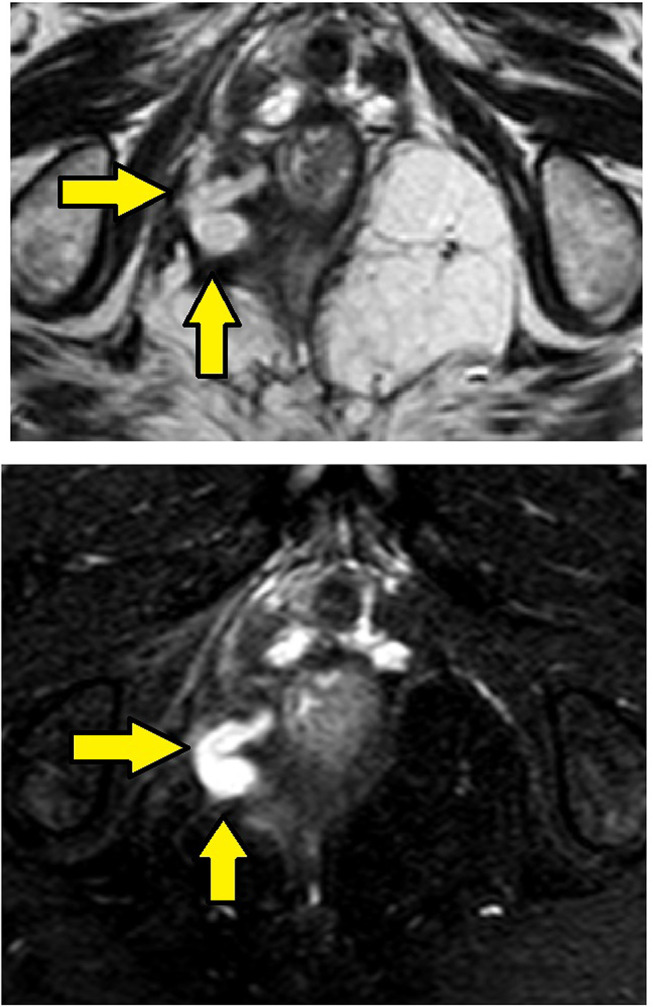
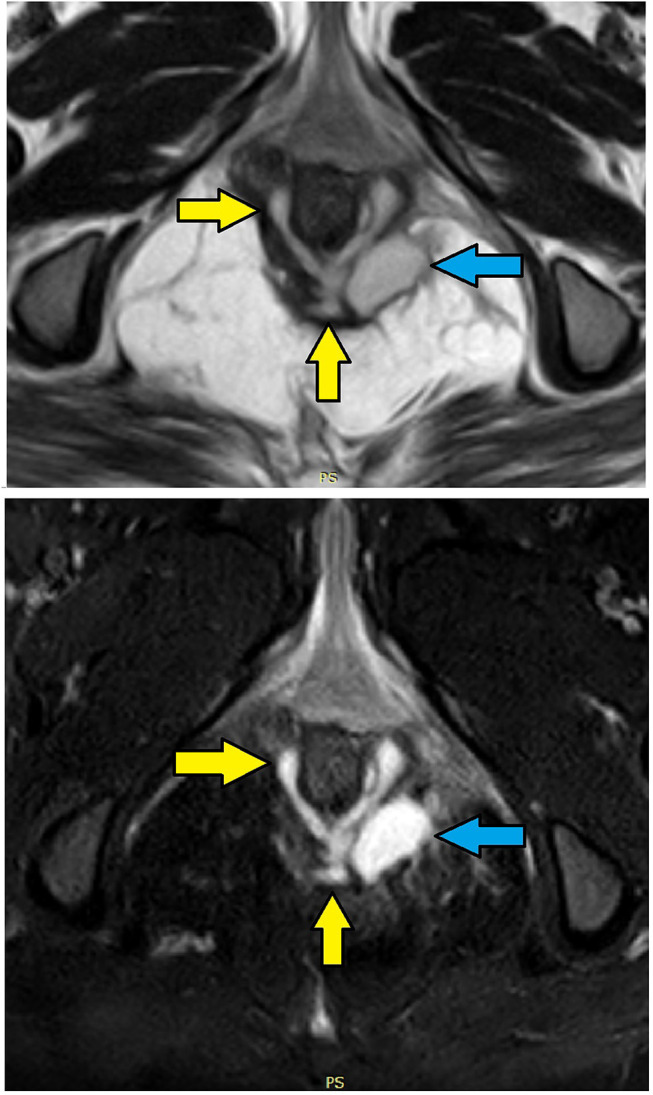
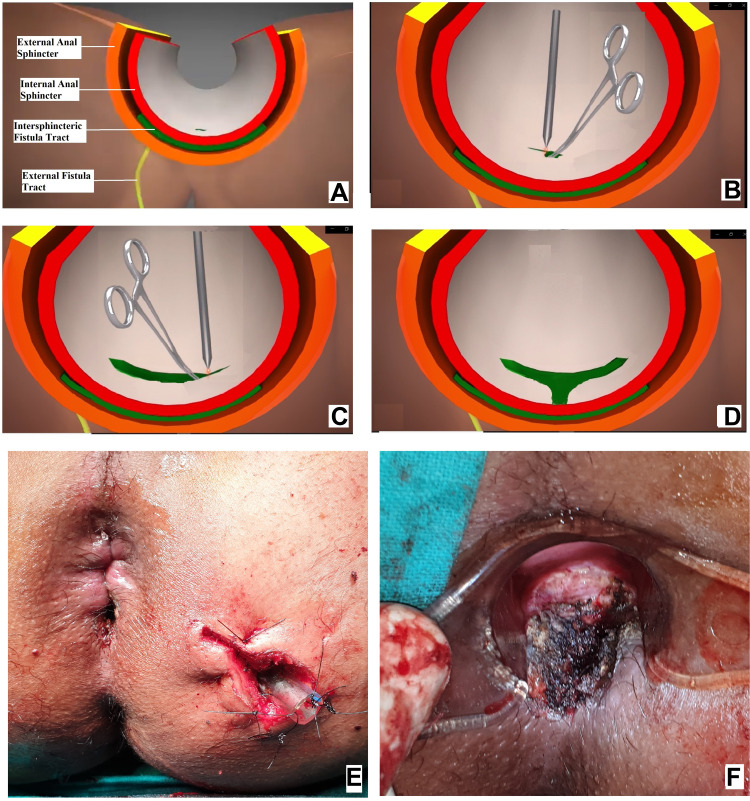
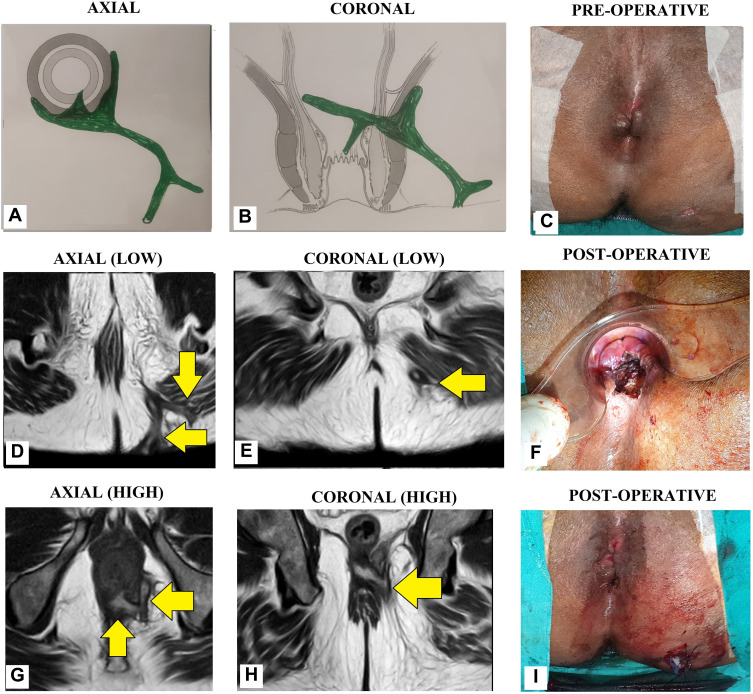
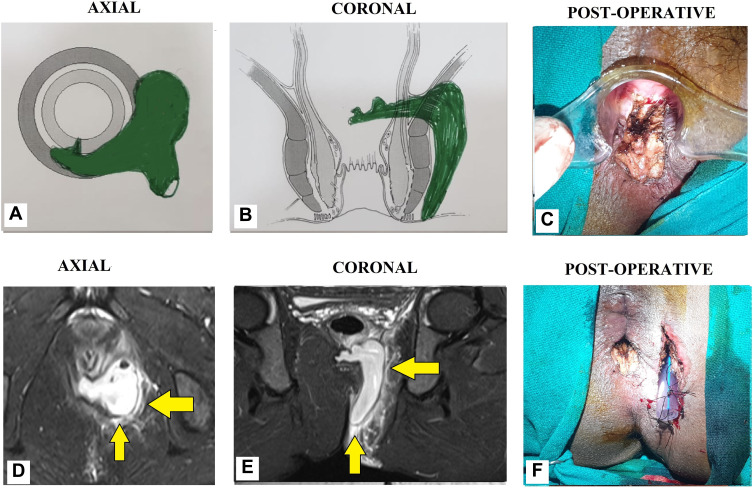
Patients and methods: All anal fistula patients operated consecutively over 7 years were included in the study. A simple two-step protocol was followed for fistulas in which the internal opening was not locatable after clinical examination and MRI assessment. First, the MRI was reassessed. The site where the fistula was closest to the internal sphincter was noted. It was assumed that the internal-opening was located at that position and the fistula was treated accordingly. Second, in horseshoe anal fistulas with no apparent internal opening, it was assumed that the internal opening was located in the midline. Low fistulas were treated by fistulotomy and high fistulas by a sphincter-sparing procedure. Incontinence was evaluated by objective incontinence scores (Vaizey scores).
Results: A total of 757 patients were operated (median follow-up-33 months). Of these, 57 patients were excluded due to short or inadequate follow-up. In 154/700 (22%) patients, the internal opening could not be located while in 546/700 (78%), the internal opening was found. Both the groups were similar in all parameters. In the "internal-opening found" group, the fistula healed completely in 486/546 (89%) and in the 'internal-opening not found group', the fistula healed in 140/156 (90.9%) (p=1.01). The objective continence scores did not change significantly after surgery in both the groups.
Conclusion: This new protocol seems effective as a high cure rate could be achieved in 'internal-opening not found' fistulas which was comparable to fistula healing in the 'internal-opening found' group.
Keywords: MRI; anal fistula; fistula-in-ano; horseshoe; internal opening; recurrence.
© 2021 Garg et al.
Conflict of interest statement
The authors report no conflicts of interest for this work.
Figures
Similar articles
-
Non-Locatable Internal Opening in Anal Fistula Associated with Acute Abscess and Its Definitive Management by Garg Protocol.Clin Exp Gastroenterol. 2022 Sep 26;15:189-198. doi: 10.2147/CEG.S374848. eCollection 2022. Clin Exp Gastroenterol. 2022. PMID: 36186926 Free PMC article.
-
Lessons learned from an audit of 1250 anal fistula patients operated at a single center: A retrospective review.World J Gastrointest Surg. 2021 Apr 27;13(4):340-354. doi: 10.4240/wjgs.v13.i4.340. World J Gastrointest Surg. 2021. PMID: 33968301 Free PMC article.
-
Transanal opening of the intersphincteric space: a novel sphincter-sparing procedure to treat 325 high complex anal fistulas with long-term follow-up.Colorectal Dis. 2021 May;23(5):1213-1224. doi: 10.1111/codi.15555. Epub 2021 Feb 19. Colorectal Dis. 2021. PMID: 33529491
-
Comparison between recent sphincter-sparing procedures for complex anal fistulas-ligation of intersphincteric tract vs transanal opening of intersphincteric space.World J Gastrointest Surg. 2022 May 27;14(5):374-382. doi: 10.4240/wjgs.v14.i5.374. World J Gastrointest Surg. 2022. PMID: 35734614 Free PMC article. Review.
-
Is simple fistula-in-ano simple?Dis Colon Rectum. 1994 Sep;37(9):885-9. doi: 10.1007/BF02052593. Dis Colon Rectum. 1994. PMID: 8076487 Review.
Cited by
-
Non-Locatable Internal Opening in Anal Fistula Associated with Acute Abscess and Its Definitive Management by Garg Protocol.Clin Exp Gastroenterol. 2022 Sep 26;15:189-198. doi: 10.2147/CEG.S374848. eCollection 2022. Clin Exp Gastroenterol. 2022. PMID: 36186926 Free PMC article.
-
The Effects of Phellodendron Decoction on Wound Healing of Anal Fistula after Anal Fistulotomy.Evid Based Complement Alternat Med. 2022 Jul 22;2022:7363006. doi: 10.1155/2022/7363006. eCollection 2022. Evid Based Complement Alternat Med. 2022. PMID: 36016687 Free PMC article.
-
The management of complex fistula in ano by transanal opening of the intersphincteric space (TROPIS): short-term results.Ann Coloproctol. 2024 Oct;40(5):474-480. doi: 10.3393/ac.2022.01018.0145. Epub 2023 Mar 31. Ann Coloproctol. 2024. PMID: 36999174 Free PMC article.
-
Efficacy and safety of transanal opening of intersphincteric space in the treatment of high complex anal fistula: A meta‑analysis.Exp Ther Med. 2024 May 31;28(2):306. doi: 10.3892/etm.2024.12595. eCollection 2024 Aug. Exp Ther Med. 2024. PMID: 38873039 Free PMC article.
-
Recent advances in the diagnosis and treatment of complex anal fistula.Ann Coloproctol. 2024 Aug;40(4):321-335. doi: 10.3393/ac.2024.00325.0046. Epub 2024 Aug 30. Ann Coloproctol. 2024. PMID: 39228196 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
