

Differential diagnosis of perinatal Bartter, Bartter and Gitelman syndromes
- PMID: 33564404
- PMCID: PMC7857843
- DOI: 10.1093/ckj/sfaa172
Differential diagnosis of perinatal Bartter, Bartter and Gitelman syndromes
Erratum in
-
Erratum: Differential diagnosis of perinatal Bartter, Bartter and Gitelman syndromes.Clin Kidney J. 2021 Jan 9;14(4):1296. doi: 10.1093/ckj/sfaa243. eCollection 2021 Apr. Clin Kidney J. 2021. PMID: 33841877 Free PMC article.
Abstract
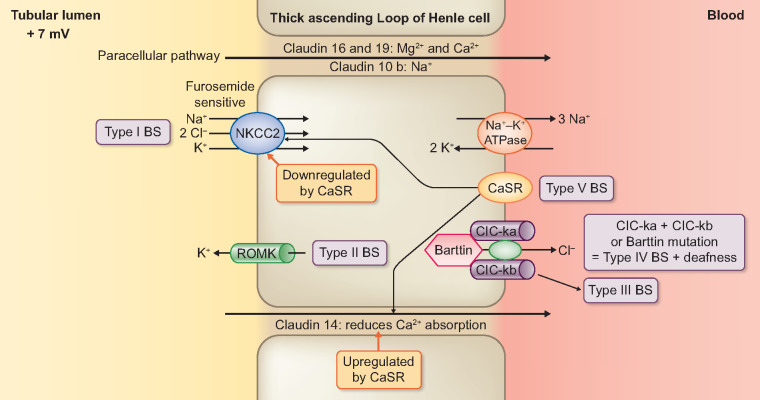
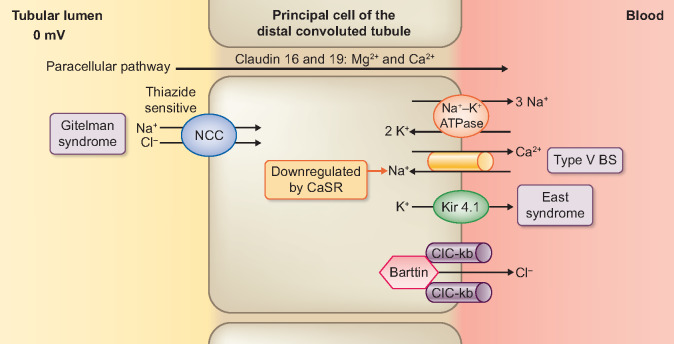
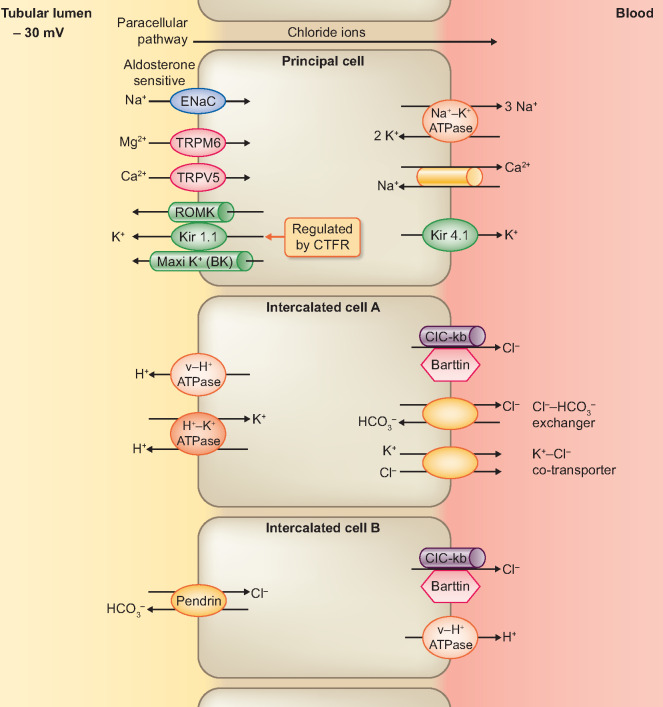
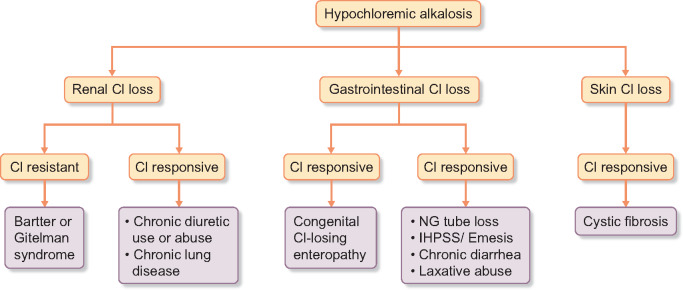
The common finding of hypokalemic alkalosis in several unrelated disorders may confound the early diagnosis of salt-losing tubulopathy (SLT). Antenatal Bartter syndrome (BS) must be considered in idiopathic early-onset polyhydramnios. Fetal megabladder in BS may allow its distinction from third-trimester polyhydramnios that occurs in congenital chloride diarrhea (CCD). Fetal megacolon occurs in CCD while fecal chloride >90 mEq/L in infants is diagnostic. Failure-to-thrive, polydipsia and polyuria in early childhood are the hallmarks of classic BS. Unlike BS, there is low urinary chloride in hypokalemic alkalosis of intractable emesis and cystic fibrosis. Rarely, renal salt wasting may result from cystinosis, Dent disease, disorders of paracellular claudin-10b and Kir4.1 potassium-channel deficiency. Acquired BS may result from calcimimetic up-regulation of a calcium-sensing receptor or autoantibody inactivation of sodium chloride co-transporters in Sjögren syndrome. A relatively common event of heterozygous gene mutations for Gitelman syndrome increases the likelihood of its random occurrence in certain diseases of adult onset. Finally, diuretic abuse is the most common differential diagnosis of SLT. Unlike the persistent elevation in BS, urinary chloride concentration losses waxes and wanes on day-to-day assessment in patients with diuretic misuse.
Keywords: Gitelman; acquired Bartter; antenatal Bartter; hypochloremic metabolic alkalosis; pseudo-Bartter syndromes.
© The Author(s) 2020. Published by Oxford University Press on behalf of ERA-EDTA.
Figures
References
-
- Simon DB, Lifton RP.. The molecular basis of inherited hypokalemic alkalosis: Bartter’s and Gitelman’s syndromes. Am J Physiol 1996; 271: F961–F966 - PubMed
-
- Seyberth HR. W, Koniger SJ, Rascher W. et al. Role of prostaglandins in hyperprostaglandin E syndrome and in selected renal tubular disorders. Pediatr Nephrol 1987; 1: 491–497 - PubMed
-
- Blanchard A, Bockenhauer D, Bolignano D. et al. Gitelman syndrome: consensus and guidance from a Kidney Disease: Improving Global Outcomes (KDIGO) controversies conference. Kidney Int 2017; 91: 24–33 - PubMed
-
- Seyberth HW, Weber S, Kömhoff M.. Bartter’s and Gitelman’s syndrome. Curr Opin Pediatr 2017; 29: 179–186 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
