

Management of patients with a failed kidney transplant: what should we do?
- PMID: 33564409
- PMCID: PMC7857798
- DOI: 10.1093/ckj/sfaa094
Management of patients with a failed kidney transplant: what should we do?
Abstract
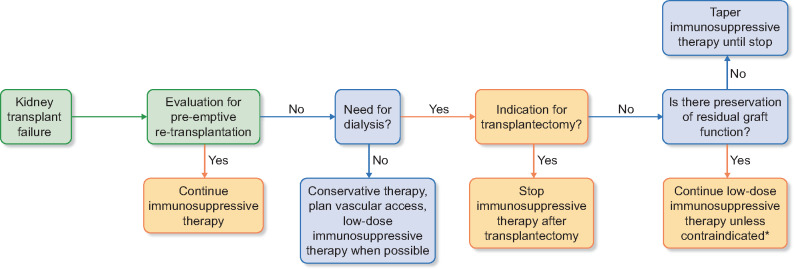
The number of kidney transplant recipients returning to dialysis after graft failure is steadily increasing over time. Patients with a failed kidney transplant have been shown to have a significant increase in mortality compared with patients with a functioning graft or patients initiating dialysis for the first time. Moreover, the risk for infectious complications, cardiovascular disease and malignancy is greater than in the dialysis population due to the frequent maintenance of low-dose immunosuppression, which is required to reduce the risk of allosensitization, particularly in patients with the prospect of retransplantation from a living donor. The management of these patients present several controversial opinions and clinical guidelines are lacking. This article aims to review the leading evidence on the main issues in the management of patients with failed transplant, including the ideal timing and modality of dialysis reinitiation, the indications for an allograft nephrectomy or the correct management of immunosuppression during graft failure. In summary, retransplantation is a feasible option that should be considered in patients with graft failure and may help to minimize the morbidity and mortality risk associated with dialysis reinitiation.
Keywords: allograft nephrectomy; allosensitization; dialysis; graft failure; immunosuppression; retransplantation.
© The Author(s) 2020. Published by Oxford University Press on behalf of ERA-EDTA.
Figures
References
-
- Laupacis A, Keown P, Pus N. et al. A study of the quality of life and cost-utility of renal transplantation. Kidney Int 1996; 50: 235–242 - PubMed
-
- Ojo AO, Hanson JA, Meier-Kriesche H. et al. Survival in recipients of marginal cadaveric donor kidneys compared with other recipients and wait-listed transplant candidates. J Am Soc Nephrol 2001; 12: 589–597 - PubMed
-
- Meier-Kriesche H-U, Schold JD, Srinivas TR. et al. Lack of improvement in renal allograft survival despite a marked decrease in acute rejection rates over the most recent era. Am J Transplant 2004; 4: 378–383 - PubMed
-
- Rao PS, Schaubel DE, Jia X. et al. Survival on dialysis post-kidney transplant failure: results from the Scientific Registry of Transplant Recipients. Am J Kidney Dis 2007; 49: 294–300 - PubMed
-
- United S Renal Data System. USRDS 2011 Annual Data Report. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2015
Publication types
LinkOut - more resources
Full Text Sources
