

Integrated immune dynamics define correlates of COVID-19 severity and antibody responses
- PMID: 33564749
- PMCID: PMC7862905
- DOI: 10.1016/j.xcrm.2021.100208
Integrated immune dynamics define correlates of COVID-19 severity and antibody responses
Abstract
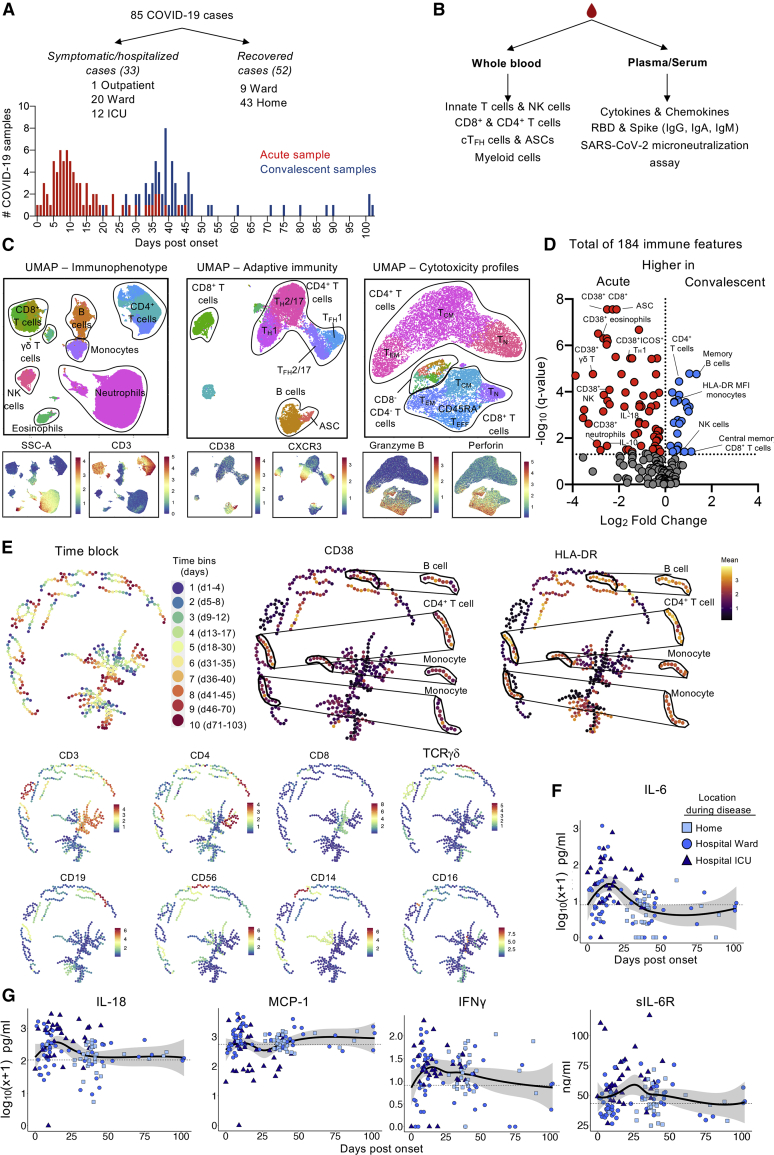
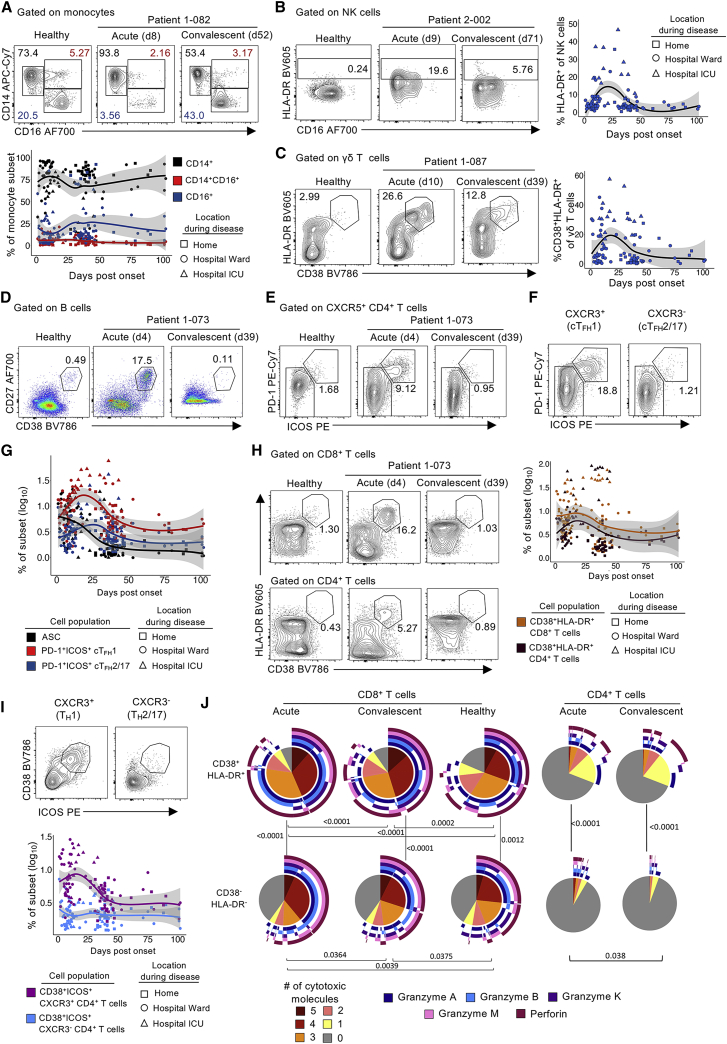
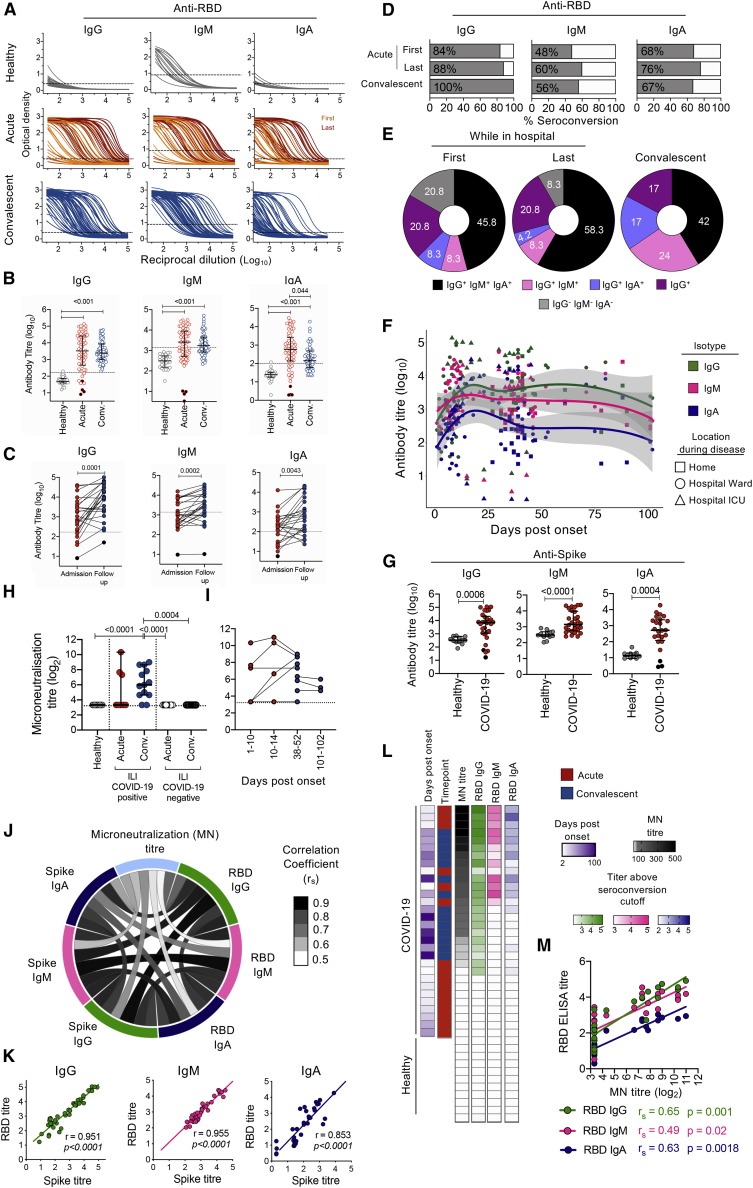
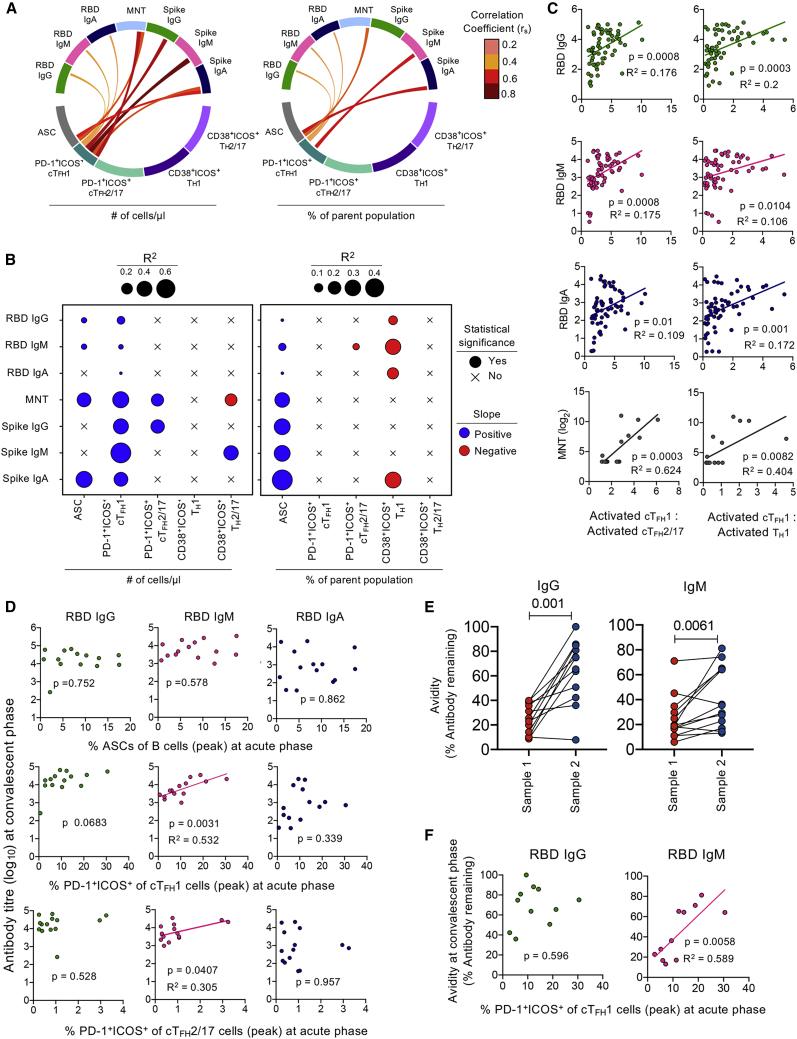
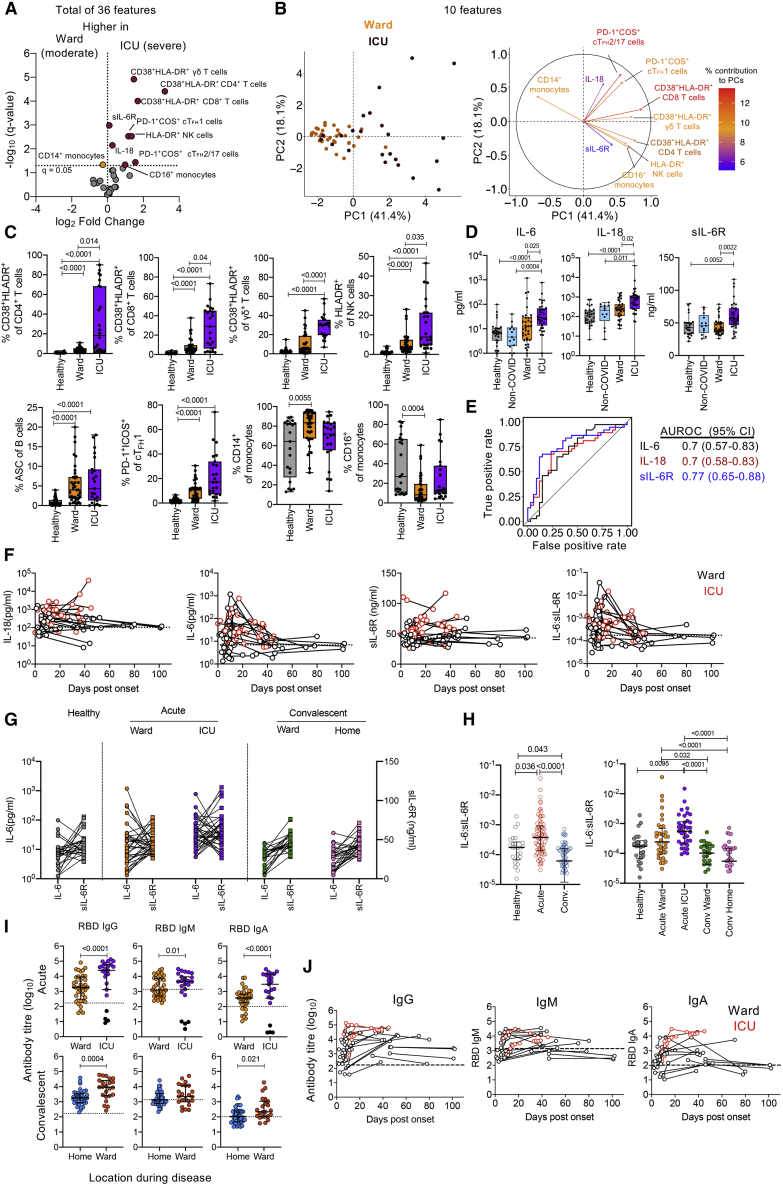
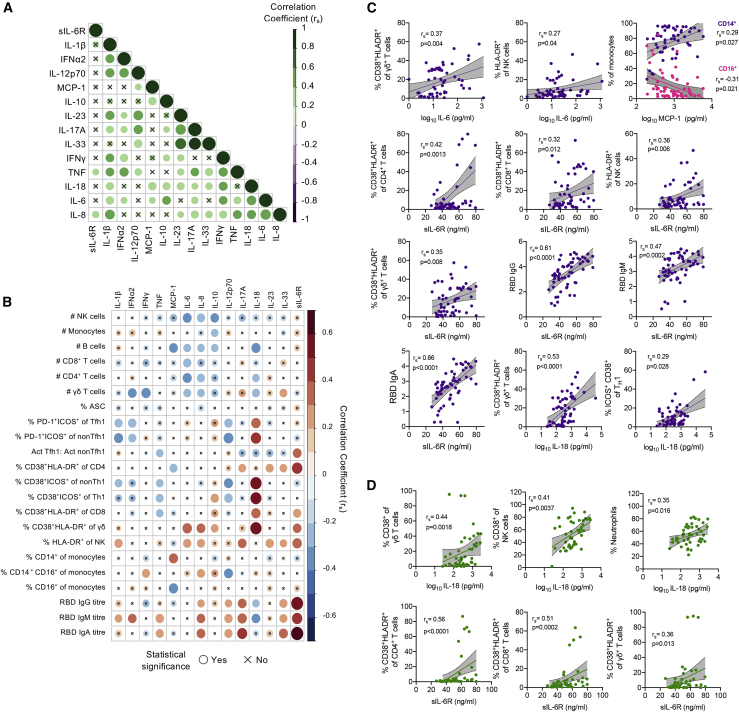
SARS-CoV-2 causes a spectrum of COVID-19 disease, the immunological basis of which remains ill defined. We analyzed 85 SARS-CoV-2-infected individuals at acute and/or convalescent time points, up to 102 days after symptom onset, quantifying 184 immunological parameters. Acute COVID-19 presented with high levels of IL-6, IL-18, and IL-10 and broad activation marked by the upregulation of CD38 on innate and adaptive lymphocytes and myeloid cells. Importantly, activated CXCR3+cTFH1 cells in acute COVID-19 significantly correlate with and predict antibody levels and their avidity at convalescence as well as acute neutralization activity. Strikingly, intensive care unit (ICU) patients with severe COVID-19 display higher levels of soluble IL-6, IL-6R, and IL-18, and hyperactivation of innate, adaptive, and myeloid compartments than patients with moderate disease. Our analyses provide a comprehensive map of longitudinal immunological responses in COVID-19 patients and integrate key cellular pathways of complex immune networks underpinning severe COVID-19, providing important insights into potential biomarkers and immunotherapies.
Keywords: CD38; HLA-DR; IL-18; IL-6; SARS-CoV-2; T follicular helper cells; acute COVID-19; antibody-secreting cells; convalescent COVID-19; soluble IL-6 receptor.
© 2021 The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Koutsakos M., Kedzierska K. A race to determine what drives COVID-19 severity. Nature. 2020;583:366–368. - PubMed
-
- Zhang X., Tan Y., Ling Y., Lu G., Liu F., Yi Z., Jia X., Wu M., Shi B., Xu S. Viral and host factors related to the clinical outcome of COVID-19. Nature. 2020;583:437–440. - PubMed
-
- Long Q.X., Tang X.J., Shi Q.L., Li Q., Deng H.J., Yuan J., Hu J.L., Xu W., Zhang Y., Lv F.J. Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections. Nat. Med. 2020;26:1200–1204. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
