

Association of Sustained Blood Pressure Control with Lower Risk for High-Cost Multimorbidities Among Medicare Beneficiaries in ALLHAT
- PMID: 33564944
- PMCID: PMC8342657
- DOI: 10.1007/s11606-021-06623-w
Association of Sustained Blood Pressure Control with Lower Risk for High-Cost Multimorbidities Among Medicare Beneficiaries in ALLHAT
Abstract
Background: Clustering of chronic conditions is associated with high healthcare costs. Sustaining blood pressure (BP) control could be a strategy to prevent high-cost multimorbidity clusters.
Objective: To determine the association between sustained systolic BP (SBP) control and incident multimorbidity cluster dyads and triads.
Design: Cohort study of Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) linked to Medicare claims.
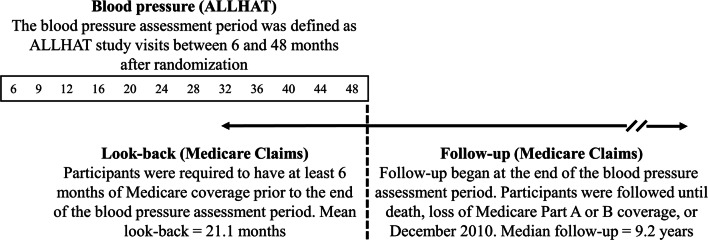
Participants: ALLHAT included adults with hypertension and ≥1 coronary heart disease risk factor. This analysis was restricted to 5234 participants with ≥ 8 SBP measurements during a 48-month BP assessment period.
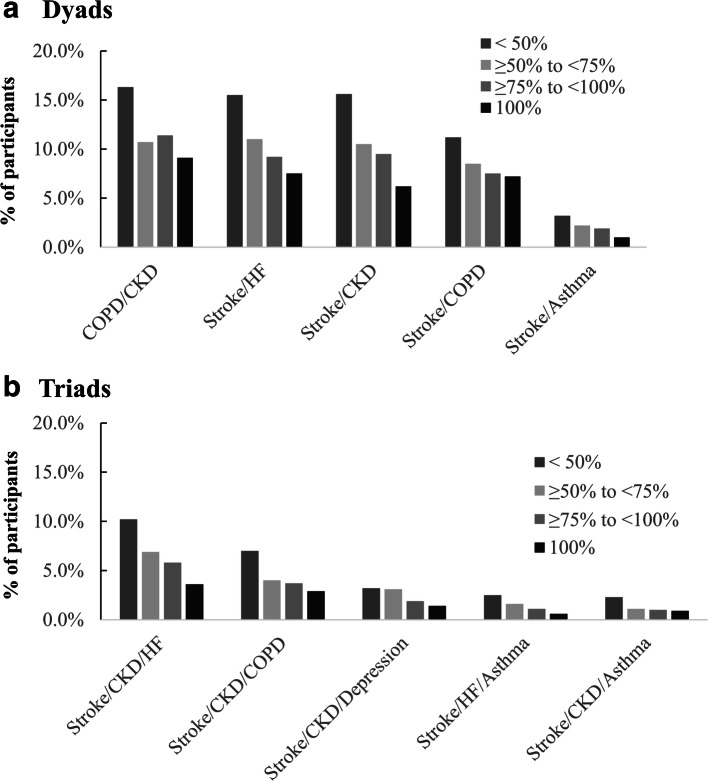
Main measures: SBP control was defined as <140 mm Hg at <50%, 50 to <75%, 75 to <100%, and 100% of study visits during the BP assessment period. High-cost multimorbidity clusters included dyads (stroke/chronic kidney disease [CKD], stroke/chronic obstructive pulmonary disease [COPD], stroke/heart failure [HF], stroke/asthma, COPD/CKD) and triads (stroke/CKD/asthma, stroke/CKD/COPD, stroke/CKD/depression, stroke/CKD/HF, stroke/HF/asthma) identified during follow-up.
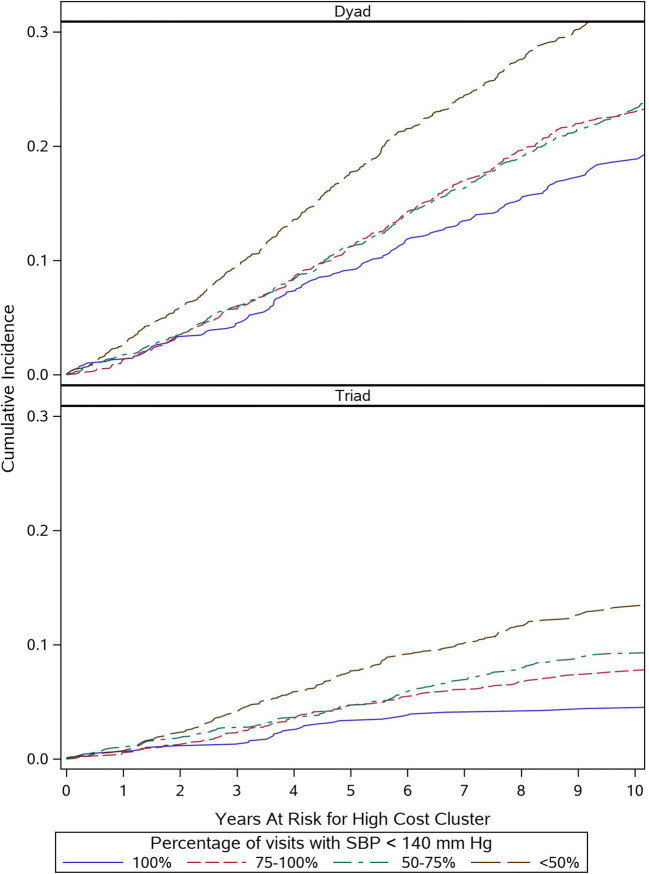
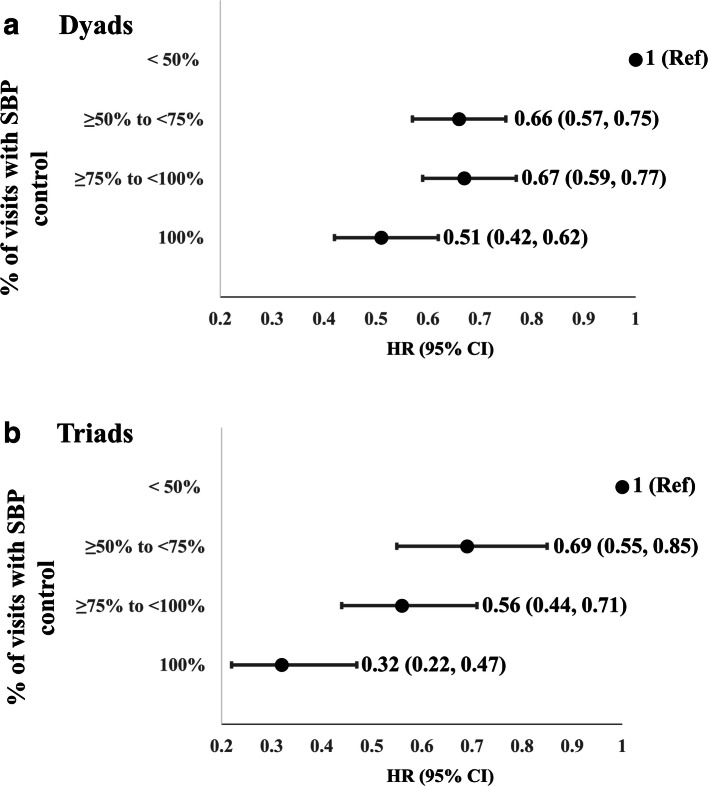
Key results: Incident dyads occurred in 1334 (26%) participants and triads occurred in 481 (9%) participants over a median follow-up of 9.2 years. Among participants with SBP control at <50%, 50 to <75%, 75 to <100%, and 100% of visits, 32%, 23%, 23%, and 19% of participants developed high-cost dyads, respectively, and 13%, 9%, 8%, and 5% of participants developed high-cost triads, respectively. Compared to those with sustained BP control at <50% of visits, adjusted HRs (95% CI) for incident dyads were 0.66 (0.57, 0.75), 0.67 (0.59, 0.77), and 0.51 (0.42, 0.62) for SBP control at 50 to <75%, 75 to <100%, and 100% of visits, respectively. The corresponding HRs (95% CI) for incident triads were 0.69 (0.55, 0.85), 0.56 (0.44, 0.71), and 0.32 (0.22, 0.47).
Conclusions: Among Medicare beneficiaries in ALLHAT, sustained SBP was associated with a lower risk of developing high-cost multimorbidity dyads and triads.
Keywords: aging; blood pressure control; hypertension; multimorbidity; systolic blood pressure.
© 2021. This is a U.S. government work and not under copyright protection in the U.S.; foreign copyright protection may apply.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
References
-
- Centers for Medicare and Medicaid Services. Chronic Conditions among Medicare Beneficiaries, Chartbook, 2012 Edition. Baltimore, MD. 2012.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
