

Targeting of the Subthalamic Nucleus in Patients with Parkinson's Disease Undergoing Deep Brain Stimulation Surgery
- PMID: 33565018
- PMCID: PMC8140007
- DOI: 10.1007/s40120-021-00233-8
Targeting of the Subthalamic Nucleus in Patients with Parkinson's Disease Undergoing Deep Brain Stimulation Surgery
Abstract
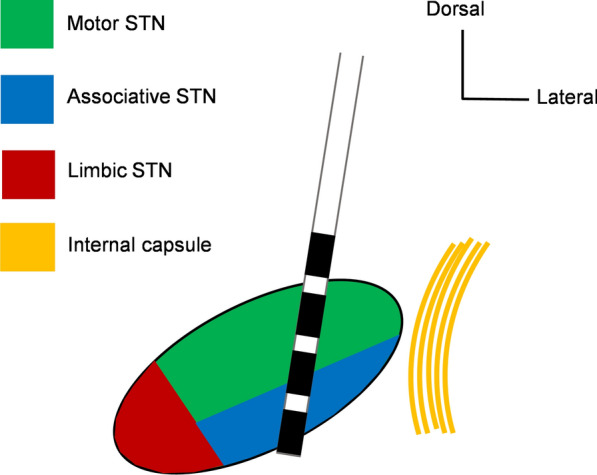
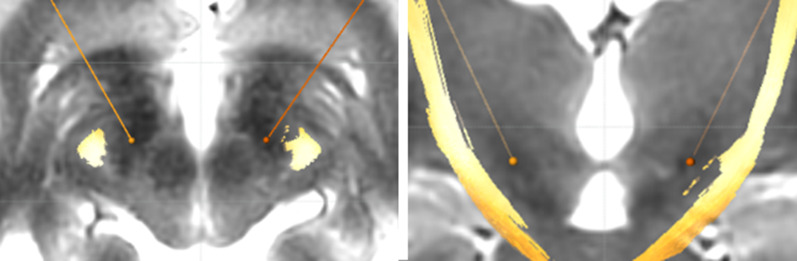
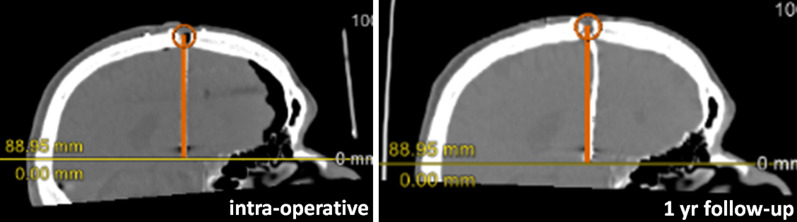
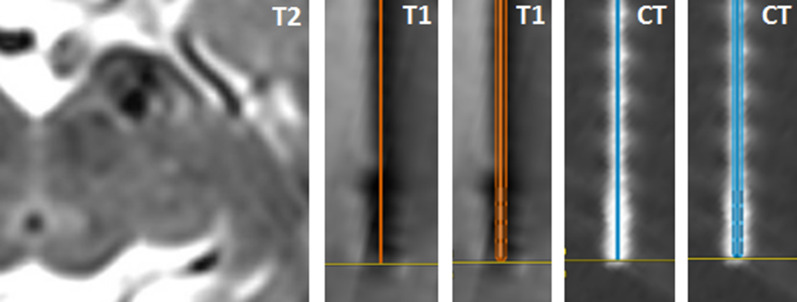
Precise stereotactic targeting of the dorsolateral motor part of the subthalamic nucleus (STN) is paramount for maximizing clinical effectiveness and preventing side effects of deep brain stimulation (DBS) in patients with advanced Parkinson's disease. With recent developments in magnetic resonance imaging (MRI) techniques, direct targeting of the dorsolateral part of the STN is now feasible, together with visualization of the motor fibers in the nearby internal capsule. However, clinically relevant discrepancies were reported when comparing STN borders on MRI to electrophysiological STN borders during microelectrode recordings (MER). Also, one should take into account the possibility of a 3D inaccuracy of up to 2 mm of the applied stereotactic technique. Pneumocephalus and image fusion errors may further increase implantation inaccuracy. Even when implantation has been successful, suboptimal lead anchoring on the skull may cause lead migration during follow-up. Meticulous pre- and intraoperative imaging is therefore indispensable, and so is postoperative imaging when the effects of DBS deteriorate during follow-up. Thus far, most DBS centers employ MRI targeting, multichannel MER, and awake test stimulation in STN surgery, but randomized trials comparing surgery under local versus general anesthesia and additional studies comparing MER-STN borders to high-field MRI-STN may change this clinical practice. Further developments in imaging protocols and improvements in image fusion processes are needed to optimize placement of DBS leads in the dorsolateral motor part of the STN in Parkinson's disease.
Keywords: Deep brain stimulation; Magnetic resonance imaging; Microelectrode recordings; Parkinson’s disease; Subthalamic nucleus; Targeting.
Figures

References
-
- Odekerken VJ, van Laar T, Staal MJ, et al. Subthalamic nucleus versus globus pallidus bilateral deep brain stimulation for advanced Parkinson’s disease (NSTAPS study): a randomised controlled trail. Lancet Neurol. 2013;12:37–44. - PubMed
-
- Benabid AL, Chabardes S, Mitrofanis J, Pollak P. Deep brain stimulation of the subthalamic nucleus for the treatment of Parkinson’s disease. Lancet Neurol. 2009;8:67–81. - PubMed
-
- Schaltenbrand G, Bailey P, editors. Introduction to stereotaxis with an atlas of the human brain. Stuttgart: George Thieme Verlag; 1959.
-
- Limousin P, Pollak P, Benazzouz A, et al. Effect on parkinsonian signs and symptoms of bilateral subthalamic nucleus stimulation. Lancet. 1995;345:91–95. - PubMed
-
- Bot M, Bour L, de Bie RM, Contarino MF, Schuurman PR, van den Munckhof P. Can we rely on susceptibility-weighted imaging for subthalamic nucleus identification in deep brain stimulation surgery? Neurosurgery. 2016;78:353–360. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
