

Contributions of cardiac dysfunction and volume status to central haemodynamics in chronic heart failure
- PMID: 33565251
- PMCID: PMC8665273
- DOI: 10.1002/ejhf.2121
Contributions of cardiac dysfunction and volume status to central haemodynamics in chronic heart failure
Abstract
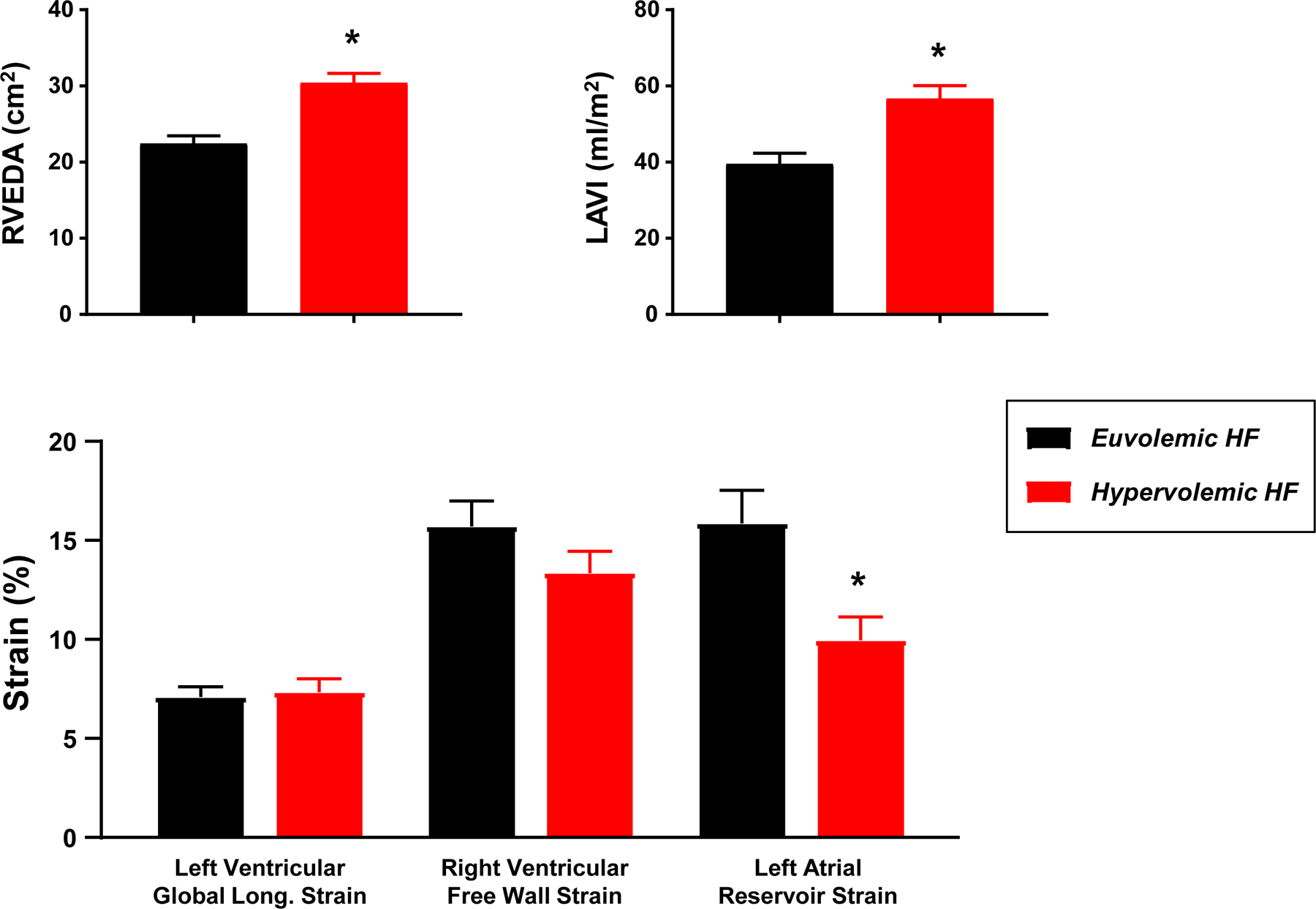
Aims: Elevated cardiac filling pressures producing clinical congestion in heart failure (HF) patients may be secondary to intravascular volume expansion or abnormalities in cardiac diastolic properties. The objective of this study was to assess the extent to which measures of myocardial function and intravascular volume correlate with haemodynamic abnormalities in chronic HF.
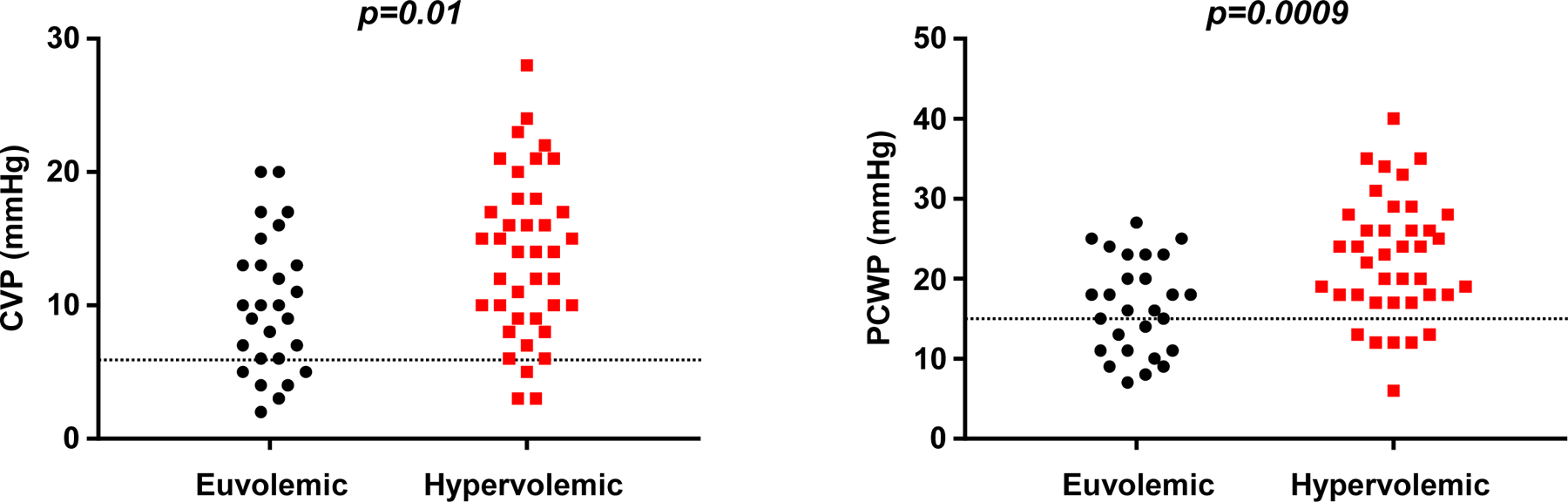
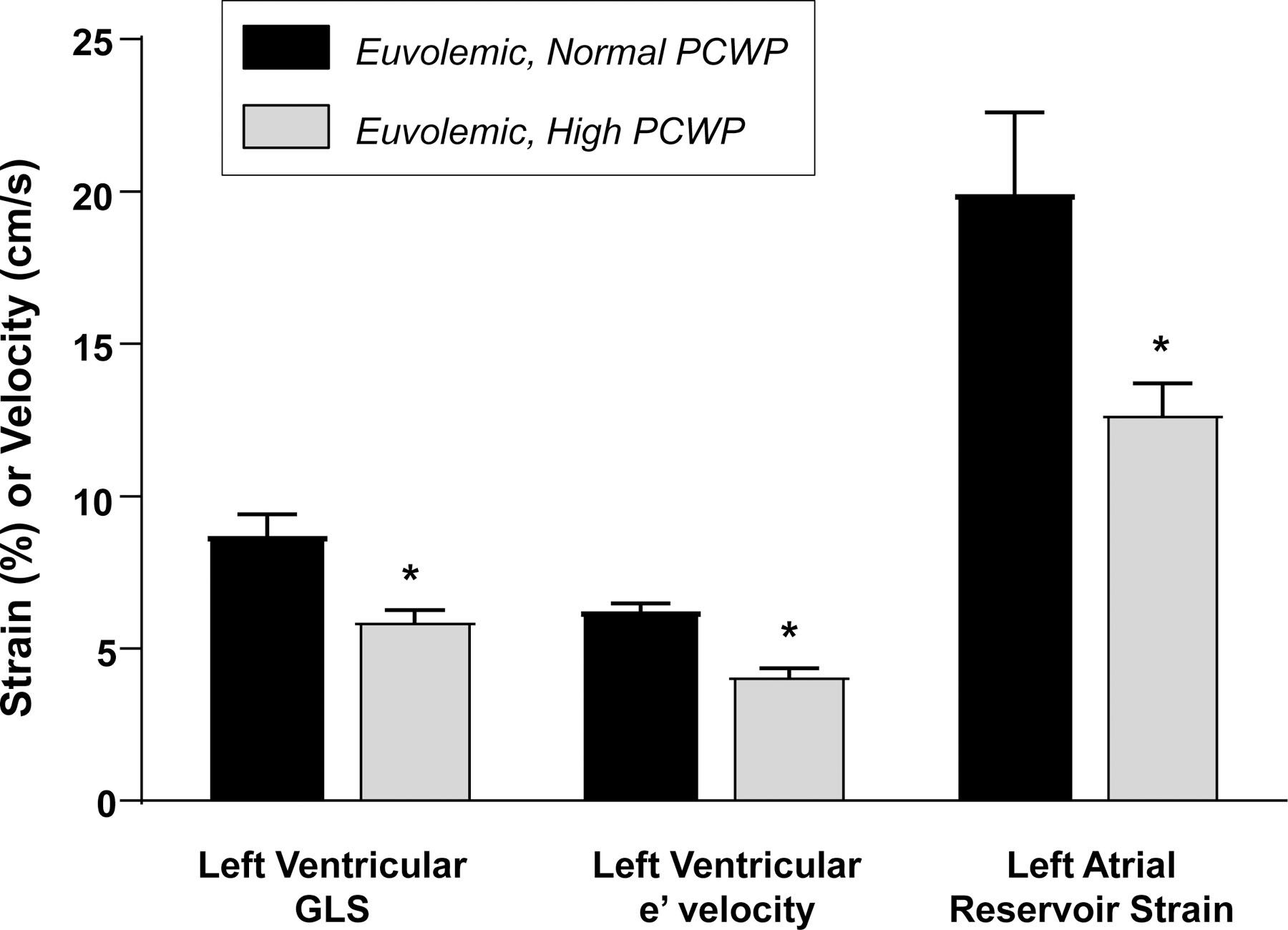
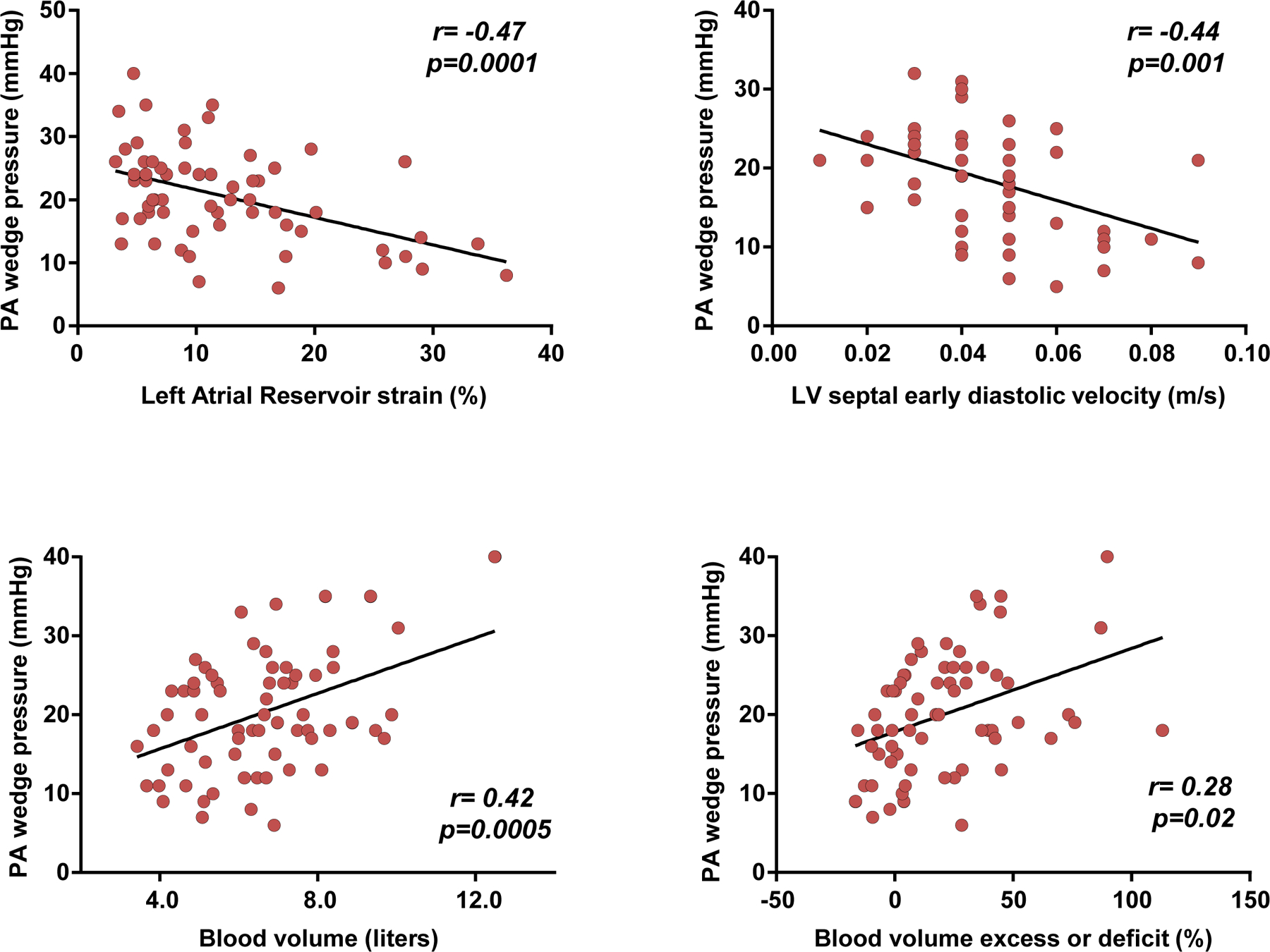
Methods and results: Subjects underwent invasive haemodynamic assessment, measurement of total blood volume (TBV) using radiolabel indicator-dilution methodology, and echocardiography to evaluate cardiac structure and function. Patients were divided into those with hypervolaemia (defined as TBV > +8% above referenced normal volume) and normal volume ('euvolaemia') (TBV ≤ + 8%). Of 66 patients, 39 (59%) were hypervolaemic and 27 (41%) normal TBV. Central venous pressure (CVP, P = 0.01) and pulmonary capillary wedge pressure (PCWP, P < 0.001) were higher in hypervolaemic compared with euvolaemic patients; however, 15% of hypervolaemic patients displayed normal pressures. Of euvolaemic patients, 70% displayed elevated CVP and 63% elevated PCWP. PCWP was moderately correlated with TBV (r = 0.42), left ventricular diastolic function (e' velocity, r = -0.44), and left atrial strain (r = -0.47). In multivariable regression TBV, left ventricular e', and left atrial strain were independently associated with PCWP (all P < 0.05).
Conclusions: While hypervolaemic patients displayed elevations in filling pressures, a substantial proportion (15%) had normal pressures, and of all subjects with elevated filling pressures nearly one third had normal TBVs. Importantly, of patients with normal volumes, a majority (>60%) display elevated filling pressures. Combined analysis of volume, pressure, and cardiac function may be helpful to guide comprehensive assessments of HF status.
Keywords: Cardiac filling pressures; Cardiac function; Heart failure; Intravascular volume.
© 2021 European Society of Cardiology.
Conflict of interest statement
Conflict of Interest
None.
Figures
Comment in
-
Not all fluid overloads are the same: some practical considerations for better decongestion.Eur J Heart Fail. 2021 Jul;23(7):1106-1109. doi: 10.1002/ejhf.2187. Epub 2021 Apr 22. Eur J Heart Fail. 2021. PMID: 33837632 No abstract available.
References
-
- Forrester JS, Water DD. Hospital treatment of congestive heart failure. Management according to hemodynamic profiles. Am J Med. 1978; 65(1):173–180. - PubMed
-
- Forrester JS, Diamond G, Chatterjee K, Swan HJ. Medical therapy of acute myocardial infarction by application of hemodynamic subsets (first of two parts). N Engl J Med. 1976; 295(24):1356–1362. - PubMed
-
- Stevenson LW. Are hemodynamic goals viable in tailoring heart failure therapy? Hemodynamic goals are relevant. Circulation. 2006; 113:1020–1027. - PubMed
-
- Binanay C, Califf RM, Hasselblad V, O’Connor CM, Shah MR, Sopko G, Stevenson LW, ESCAPE Investigators, ESCAPE study coordinators. Evaluation study of congestive heart failure and pulmonary artery catheterization effectiveness: The ESCAPE Trial. JAMA. 2005; 294(13):1625–1633. - PubMed
-
- Levey AS, Coresh J, Balk E, Kausz AT, Levin A, Steffes MW, Hogg RJ, Perrone RD, Lau J, Eknoyan G. National Kidney Foundation practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Ann Intern Med. 2003;139:137–147. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
