

Cervical Cancer in Sub-Saharan Africa: A Multinational Population-Based Cohort Study of Care and Guideline Adherence
- PMID: 33565668
- PMCID: PMC8100544
- DOI: 10.1002/onco.13718
Cervical Cancer in Sub-Saharan Africa: A Multinational Population-Based Cohort Study of Care and Guideline Adherence
Abstract
Background: Cervical cancer (CC) is the most common female cancer in many countries of sub-Saharan Africa (SSA). We assessed treatment guideline adherence and its association with overall survival (OS).
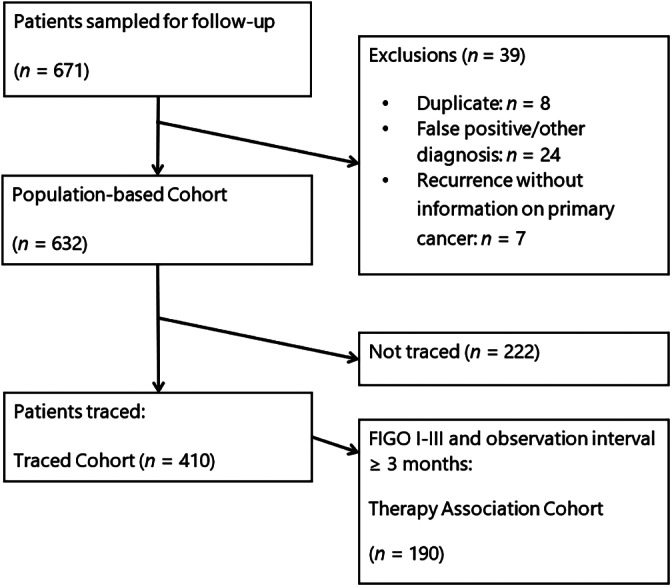
Methods: Our observational study covered nine population-based cancer registries in eight countries: Benin, Ethiopia, Ivory Coast, Kenya, Mali, Mozambique, Uganda, and Zimbabwe. Random samples of 44-125 patients diagnosed from 2010 to 2016 were selected in each. Cancer-directed therapy (CDT) was evaluated for degree of adherence to National Comprehensive Cancer Network (U.S.) Guidelines.
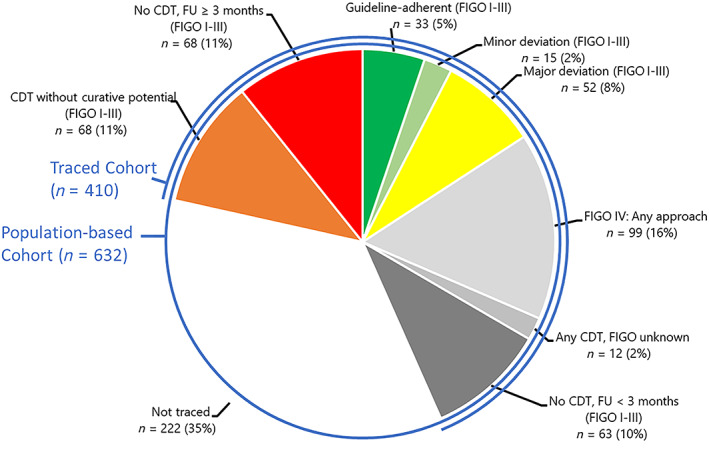
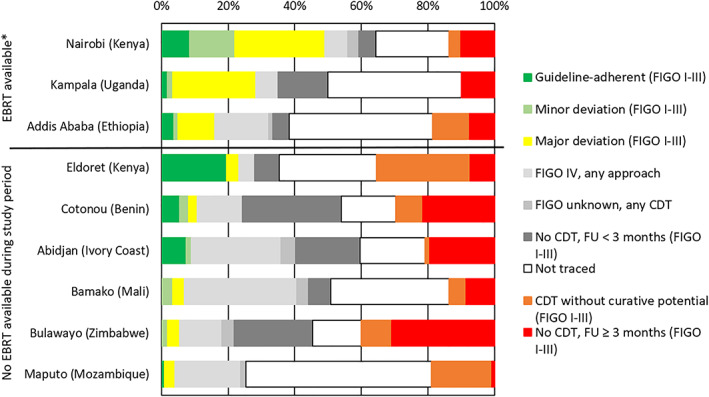
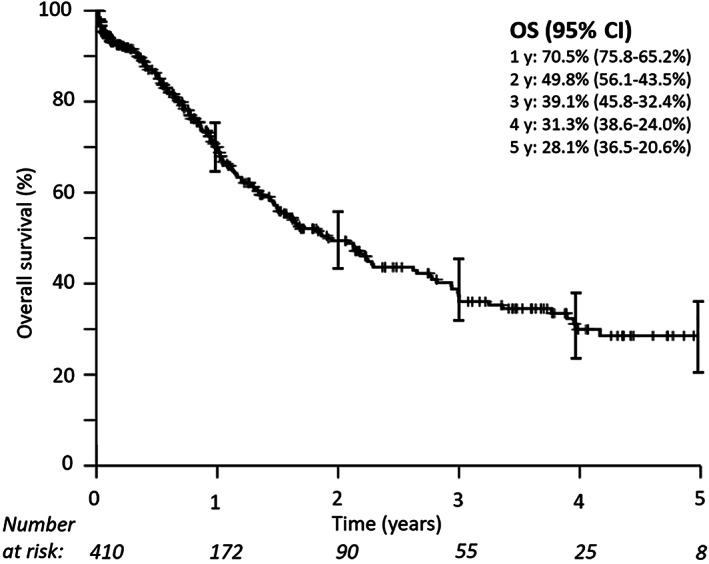
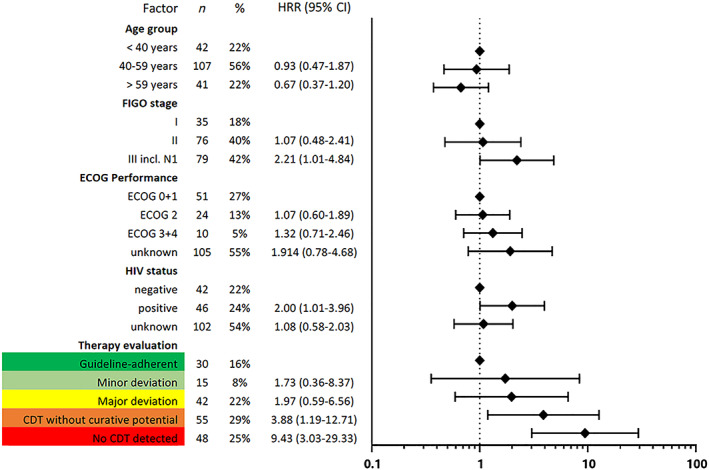
Results: Of 632 patients, 15.8% received CDT with curative potential: 5.2% guideline-adherent, 2.4% with minor deviations, and 8.2% with major deviations. CDT was not documented or was without curative potential in 22%; 15.7% were diagnosed with International Federation of Gynecology and Obstetrics (FIGO) stage IV disease. Adherence was not assessed in 46.9% (no stage or follow-up documented, 11.9%, or records not traced, 35.1%). The largest share of guideline-adherent CDT was observed in Nairobi (49%) and the smallest in Maputo (4%). In patients with FIGO stage I-III disease (n = 190), minor and major guideline deviations were associated with impaired OS (hazard rate ratio [HRR], 1.73; 95% confidence interval [CI], 0.36-8.37; HRR, 1.97; CI, 0.59-6.56, respectively). CDT without curative potential (HRR, 3.88; CI, 1.19-12.71) and no CDT (HRR, 9.43; CI, 3.03-29.33) showed substantially worse survival.
Conclusion: We found that only one in six patients with cervical cancer in SSA received CDT with curative potential. At least one-fifth and possibly up to two-thirds of women never accessed CDT, despite curable disease, resulting in impaired OS. Investments into more radiotherapy, chemotherapy, and surgical training could change the fatal outcomes of many patients.
Implications for practice: Despite evidence-based interventions including guideline-adherent treatment for cervical cancer (CC), there is huge disparity in survival across the globe. This comprehensive multinational population-based registry study aimed to assess the status quo of presentation, treatment guideline adherence, and survival in eight countries. Patients across sub-Saharan Africa present in late stages, and treatment guideline adherence is remarkably low. Both factors were associated with unfavorable survival. This report warns about the inability of most women with cervical cancer in sub-Saharan Africa to access timely and high-quality diagnostic and treatment services, serving as guidance to institutions and policy makers. With regard to clinical practice, there might be cancer-directed treatment options that, although not fully guideline adherent, have relevant survival benefit. Others should perhaps not be chosen even under resource-constrained circumstances.
Keywords: Access to care; Cervical cancer; Population-based; Radiotherapy; Sub-Saharan Africa; Survival.
© 2021 The Authors. The Oncologist published by Wiley Periodicals LLC on behalf of AlphaMed Press.
Conflict of interest statement
Figures
References
-
- Bach PB. Using practice guidelines to assess cancer care quality. J Clin Oncol 2005;23:9041–9043. - PubMed
-
- Devesa SS, Silverman DT. Cancer incidence and mortality trends in the United States: 1935‐74. J Natl Cancer Inst 1978;60:545–571. - PubMed
-
- Bray F, Ferlay J, Soerjomataram I et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68:394–424. - PubMed
-
- United Nations, Department of Economic and Social Affairs, Population Divison (2017). World Population Prospects: The 2017 Revision, custom data acquired via website. Available at: https://population.un.org/wpp/Publications/. Accessed February 18, 2019.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
